

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastric cancer is a major health issue, the 5th most common malignancy, and third leading cause of cancer-related death worldwide, according to GLOBOCAN 2012 [1]. Although the standard treatment for gastric cancer is surgical resection of the stomach with radical lymphadenectomy, excessive lymph node (LN) dissection increases patient morbidity and mortality, and gastrectomy itself decreases the quality of life of patients with gastric cancer. Therefore, if we can predict the LN metastasis status before or during the operation, a tailored gastrectomy, such as a wedge resection or limited LN dissection, would be possible, especially for early cancer.
Sentinel lymph node (SN) biopsies for predicting metastatic LNs have been widely used in breast cancer and melanoma. However, the clinical application of SN biopsies for gastric cancer has been challenging, due to complicated multidirectional lymphatic drainage around the stomach, and the risk of skip metastasis or false-negative intraoperative histological examinations in gastric cancer [23]. SN biopsy methods and techniques have gradually evolved for gastric cancer, and a recent Japanese study showed promising results in SN navigation surgery detection and sensitivity [4]. In Korea, the SENtinel NOde ORIented Tailored Approach (SENORITA) study group planned a multicenter phase III trial that compared conventional laparoscopic gastrectomy to laparoscopic SN biopsy with limited gastrectomy in patients with clinical stage Ia gastric cancer. Before beginning this phase III trial, we performed a quality control study to qualify the institutions that were participating in the phase III trial and to standardize the surgical procedures [5].
SN biopsy in gastric cancer is a difficult procedure, with a steep learning curve [6]. Many factors, such as endoscopic dual tracer injection into the submucosa, detection of the SN basin that is hidden under perigastric fat tissues, successful sentinel basin dissection (SBD) without major bleeding or gastric wall injury, and SN identification at the back table affect the outcomes of successful sentinel lymph node navigation surgery (SNNS). In particular, avoiding postoperative complications that are related to the SBD procedure is important for the early recovery of patients and the continuous application of SNNS. Therefore, in this quality control study, we investigated the operative and postoperative complications, to clarify the safety of the SBD procedure.
MATERIALS AND METHODS
We have previously described the methods of this prospective, multicenter feasibility quality control trial in detail [57].
We enrolled patients with gastric cancer who were between 20 and 80 years of age and of clinical stage T1-2N0M0, according to the American Joint Committee on Cancer (AJCC), 7th edition [8]. Indications for this prospective, multicenter quality control trial included that the longest tumor diameter was less than 4 cm, under endoscopic measurement, and the tumor was located at least 2 cm from the pylorus or cardia. Patients who had absolute indications for endoscopic submucosal dissection (ESD) were excluded in this study. Totally 7 institutions of SENORITA study group participated in this prospective quality control trial, and all data from patients were registered in a central data center (eVelos System; Velos, Inc., Fremont, CA, USA). Before the laparoscopic SBD surgery, all patients provided written informed consent. All participating institutions had approval by the local Institutional Review Boards for this study. (approval number: D-1201-002-002 at the institution of corresponding author)
A minimum of 10 cases of success for all 7 steps were required at each institution, for participation in the subsequent phase III trial for qualification into this study. The success for each case in this quality control trial means the completion of 7 steps for assessing the adequacy of the procedure that were performed by the endoscopists, surgeons, and pathologists in each institution [57]. Step 1 testifies which the tracer was injected by intraoperative esophagogastroduodenoscopy (EGD) at the submucosal layer or not. Step 2 involves the intraoperative EGD tracer injection at adequate 4 sites. Step 3 is assessment of the presence or absence of intraluminal or extraluminal tracer leakage, during intraoperative EGD injection. Step 4 means the injection of tracers by intraoperative EGD within 3 minutes from the first to the fourth injection. Step 5 is the intraoperative laparoscopic identification of at least one SB. Step 6 indicates which the SBNs were evaluated by intraoperative frozen biopsy or not. Lastly, step 7 is the identification of at least 5 isolated SBNs, and the analysis of frozen sections.
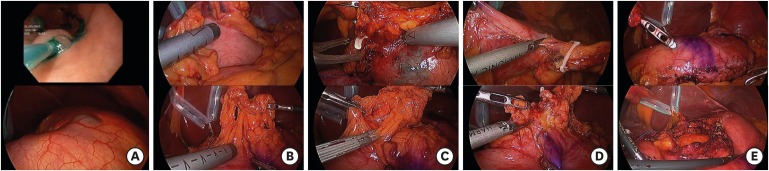
Fig. 1 illustrates the SBD procedure. To detect SNs, a mixture of indocyanine green (ICG; Diagnogreen1, 2 mL, 5 mg/mL, Daiichi-Sankyo Co., Ltd., Tokyo, Japan) and human serum albumin with radiolabel (Tc99m-HSA; 2 mL, 0.1 mCi/mL) was used as a dual tracer. In the first step of the surgery, the dual tracer was injected into the submucosal layer, in the 4 quadrants of the gastric tumor (1 mL at each quadrant, for a total volume of 4 mL), via an intraoperative endoscopic approach. During the endoscopic injections, we laparoscopically monitored the serosal layer of the stomach, to prevent intragastric or intraperitoneal tracer leakage. Fifteen minutes after endoscopic injection of the dual tracer, stained lymphatic vessels and LNs were identified. Afterward, a laparoscopic handheld gamma probe was applied to detect radioactive SNs. At this time, each side of the stomach and the lesser and greater curvature sites were meticulously assessed. The sentinel basin (SB) margins were marked by laparoscopic clips. SBs containing SNs were carefully dissected, within the marked sites, and retrieved from the surgical field. The harvested SBs were dissected, to isolate LNs. All isolated LNs from the SBs were defined as sentinel basin nodes (SBNs), which refer to LNs located completely within the SB.
Fig. 1
The steps of laparoscopic SBD. (A) Endoscopic injection of Tc99m-HSA with ICG and a laparoscopic view after tracer injection. (B) Laparoscopic sentinel basin node detection along the greater and lesser curvatures of the stomach. (C) Surgical clip application for marking the extent of laparoscopic SBD in the greater and lesser curvatures of the stomach. (D) Laparoscopic SBD along the greater and lesser curvatures of the stomach. (E) Completion of laparoscopic SBD along the greater and lesser curvatures of the stomach.
SBD = sentinel basin dissection; ICG = indocyanine green.
SBNs were classified into 4 types of SBNs: hot node (HN), green node (GN), both hot and green node (HGN), and basin node (BN), as described in our previous report [57]. The GN shows only ICG uptake, without Tc99m-HSA, HN shows 99mTc-HSA uptake, without ICG staining, and HGN presents concurrent uptake of ICG and 99mTc-HSA. A BN is a non-sentinel node that is located within the same SB. In other words, LNs retrieved from an SB that were neither green nor hot were defined as BNs. All SBNs were extracted during surgery and sent to a pathologist for intraoperative frozen sectioning. LNs that were harvested from the SBs were histologically examined intraoperatively, with hematoxylin and eosin (H&E) staining, using a single, cut plane of a frozen section. Standard gastrectomy, with lymphadenectomy of D1+ or more, was performed after SBD in all patients, according to the Japanese gastric cancer treatment guidelines [9]. After conventional surgery, the remaining LNs were classified by LN station, according to the anatomical definition of the Japanese guidelines, and sent for permanent pathologic examination by H&E staining [10].
All of SBD procedure-related or surgical complication data from the Korean multicenter prerequisite quality control trial were classified according to the Clavien-Dindo Classification (CDC) [511]. Also, the data were compared to the results of another multicenter prospective SNNS trial, which demonstrated the feasibility of gastric cancer SN mapping with the dual tracer method in Japan [4].
RESULTS
Among the 112 patients who were preoperatively enrolled at 7 institutions, 4 were excluded because of screening failures, 2 withdrew after enrollment, 1 had double primary cancer, and 1 had poor bowel preparation for the intraoperative endoscopic procedure. Consequently, 108 patients were eligible for the final analyses, 8 of whom (7.4%) experienced postoperative complications in the early postoperative period, within 30 days after surgery.
Table 1 shows the details of the 8 cases with complications, which included 1 with duodenal stump leakage, 2 with pancreatitis, 3 with gastric stasis, 1 with ileus, and 1 with bleeding. The patient with duodenal stump leakage recovered after percutaneous drainage and was classified with a grade IIIa complication, under the CDC. The other complications were mild and recovered with supportive care. There were no complications directly related to the SBD procedure, and there were no cases of mortality. In addition, there were no serious allergic reactions during or after tracer injection after surgery. Intraoperative endoscopic injections were completely performed within 3 minutes in all of the cases with complications. The average hospital stay length of the 8 cases with complications was 13.1 days. For the patient with duodenal stump leakage, the length of hospital stay was 23 days, which was the longest of the 8 complications.
Table 1
Details of the 8 cases with complications
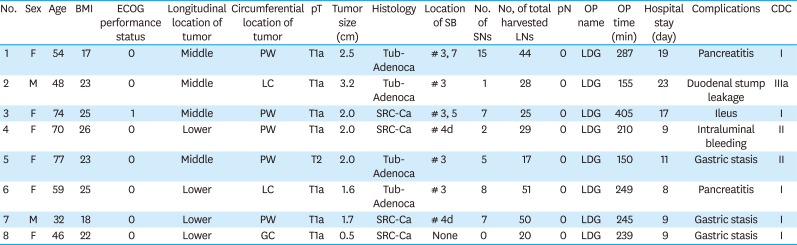
BMI = body mass index; ECOG = Eastern Cooperative Oncology Group; PW = posterior wall; LC = lesser curve; GC = greater curve; Tub-Adenoca = tubular adenocarcinoma; SRC-Ca = signet-ring cell carcinoma; SB = sentinel basin; SN = sentinel lymph node; LN = lymph node; LDG = laparoscopic distal gastrectomy; OP = surgery; CDC = Clavien-Dindo Classification.
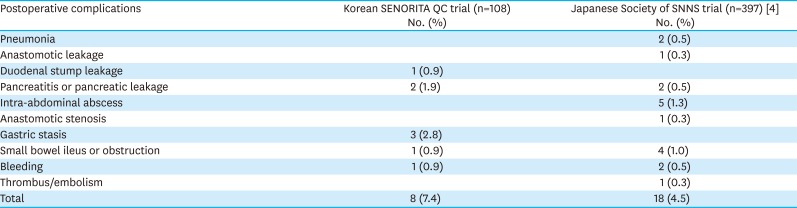
In Table 2, we compare our surgical complication results to those of the Japanese SNNS trial [4]. The incidence of postoperative complications was 7.4% (8/108) in our study and 4.5% (18/397) in the Japanese SNNS trial. In the Japanese study, intraabdominal abscesses and small bowel ileuses were common complications, followed by pneumonia, bleeding, anastomotic leakage, stenosis, and thrombus or embolism. The Japanese SNNS trial did not report any abnormal reactions that were related to dual tracer injections.
Table 2
Comparison of complications that were observed in the Japanese Society of SNNS and Korean SENORITA QC trials
| Postoperative complications | Korean SENORITA QC trial (n=108) No. (%) | Japanese Society of SNNS trial (n=397) [4] No. (%) |
|---|---|---|
| Pneumonia | 2 (0.5) | |
| Anastomotic leakage | 1 (0.3) | |
| Duodenal stump leakage | 1 (0.9) | |
| Pancreatitis or pancreatic leakage | 2 (1.9) | 2 (0.5) |
| Intra-abdominal abscess | 5 (1.3) | |
| Anastomotic stenosis | 1 (0.3) | |
| Gastric stasis | 3 (2.8) | |
| Small bowel ileus or obstruction | 1 (0.9) | 4 (1.0) |
| Bleeding | 1 (0.9) | 2 (0.5) |
| Thrombus/embolism | 1 (0.3) | |
| Total | 8 (7.4) | 18 (4.5) |
DISCUSSION
The incidence of complications was 7.4% (8/108), and only one grade IIIa complication developed in this quality control study for laparoscopic SBD. In addition, there were no cases of allergic reactions after tracer injections. Considering that all patients recovered successfully, the SBD procedure appears safe and without additional risks.
In gastric cancer, SBD, which is also called sentinel lymphatic basin dissection, has been reported to be better than the pick-up method for successful SNNS [1213]. The detection rate of SNs was determined to be 54.8% by the pick-up method and 96% by SBD [14]. Therefore, the SENORITA study in Korea and the Japanese prospective multicenter trial performed the SBD procedure for SNNS. Also, we anticipate that SBD will be the standard surgical procedure for SNNS in the future. In addition, even though our study was a quality control trial that took place prior to the phase III trial, our data support the successful and safe completion of the phase III trial.
In the previous Japanese study, there was no significant increase in the number of postoperative complications that were caused by the SN biopsy procedures, and no serious allergic reactions were observed after tracer injection. The authors observed only transient pigmentation (0.3%) and decreased pulse oximeter oxygen saturation (0.8%) [4]. ICG is a widely used material for determining cardiac output, hepatic function, and liver blood flow and is commonly used in ophthalmic angiographies. It is also used for SN mapping in breast cancer, malignant melanoma, and gastrointestinal tumors. The allergic reactions to ICG include facial flushing, hypotension, tachycardia, urticaria, pruritus, dyspnea, and anaphylactic shock, which rarely develop when ICG is injected with incomplete dissolution [15]. The maximum radiation dose of Tc99m-HSA that was used in this study was 0.4 mCi, which is only 1.3% of the 30 mCi that is commonly performed for bone scans [16]. However, because radioisotope usage has some disadvantages, such as high cost, radioactivity, and handling difficulty, ICG fluorescence imaging SN mapping has been recently introduced for SNNS in gastric cancer [1718].
A previous analysis of the Korean surgery study group trial found that the immediate postoperative morbidity was 11.6%, after laparoscopy-assisted distal gastrectomy [19]. Also, a retrospective multicenter study of laparoscopic gastrectomy by the Japanese and Korean laparoscopic surgery study groups reported morbidity rates of 14.8% and 15.1%, respectively [2021]. Although a relatively small number of patients was enrolled in the present study, the incidence of complication (7.4%, 8/108) was similar or less than other studies. In this quality control study, all patients underwent conventional laparoscopic gastrectomy with D1+ or more LN dissections. We observed a few complications that were derived only from conventional gastrectomy, and no additional risks were associated with the dual tracer injection and SBD procedures.
The SENORITA multicenter, phase III, randomized control trial for individualized function-preserving gastrectomies, including gastric wedge resection, segmental gastrectomy, and intraoperative ESD with SBD for T1N0 gastric cancer, is currently underway in Korea [2223]. Even though the surgical complications for laparoscopic-limited function-preserving gastrectomies, such as wedge resection, segmental resection, or partial gastrectomy, could not be evaluated in this quality control study, we will report the SBD procedure and surgery-related complications from the SENORITA trial in the near future.
In conclusion, no complications were directly related to the laparoscopic SBD procedures that were performed in our study. Laparoscopic SBD is a safe procedure, based on the results of our prospective, multicenter feasibility quality control trial, which was performed prior to the phase III trial.
 XML Download
XML Download