

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastric cancer remains the third leading cause of cancer-related deaths worldwide, despite substantial decreases in incidence in most areas of the world [1]. Currently, Korea has the highest global incidence of gastric cancer (41.4 per 100,000). However, the implementation of nationwide health screening programs and improved diagnostic techniques have led to steady increases in early gastric cancer diagnosis. Accordingly, the proportion of T1 cancers has increased consistently, with such cases now accounting for >60% of all gastric cancers in Korea [2].
Malnutrition is among the main postoperative complications of radical subtotal or total gastrectomy for gastric cancer [345] and is an important outcome, given the influence of the nutritional status on a patient's quality of life, morbidity, and mortality [6]. Malnutrition plays a particularly important role in the overall survival of patients with malignant tumors: a poorer nutritional status increases infection susceptibility, delays wound healing, impairs blood clotting, induces vessel wall fragility, and directly increases postoperative complications [789]. Malnutrition can also promote tumor development by suppressing tumor immunity [10].
Although many researchers consider malnutrition an unavoidable complication, the nutritional consequences of gastrectomy remain poorly investigated. To date, studies of dietary lifestyles after gastric surgery for gastric cancer have largely focused on short-term nutritional outcomes [61112]. In addition, these studies have also concentrated on total gastrectomy; accordingly, little is known about the long-term nutritional outcomes of patients treated via distal gastrectomy. The latter procedure has become increasingly feasible as a result of advances in surgical techniques and chemotherapy, and long-term outcome data are becoming available as a result of the increased population of long-term survivors. The present study aimed to determine whether patients who undergo total or distal gastrectomy, and who do and do not undergo postoperative adjuvant chemotherapy should be monitored for malnutrition.
MATERIALS AND METHODS
Patients
The protocol of this single-center retrospective cohort study was approved by the Internal Review Board of the Seoul National University Bundang Hospital, Seongnam, Korea, an academic hospital affiliated with the Seoul National University College of Medicine (Approval No. L-20151223). The requirement for informed consent from the patients was waived because of the retrospective nature of this study. This study was conducted according to the principles of the Declaration of Helsinki.
The study cohort comprised all consecutive patients with gastric cancer who underwent curative gastrectomy at Seoul National University Bundang Hospital from January 2008 to December 2009. The patients' medical records, which were collected prospectively, were reviewed retrospectively at Seoul National University Bundang Hospital. Only patients who had been followed up for ≥5 years were included. Patients who died, were lost to follow-up, or developed a recurrence within 5 years postoperatively were excluded.
The patients were divided into 2 groups according to whether they underwent total or distal gastrectomy. In a separate analysis, the patients were divided according to whether they did or did not receive postoperative adjuvant chemotherapy, comprising either titanium silicate-1 chemotherapy for 12 months, or a combination of capecitabine and oxaliplatin for 6 months. In a third analysis, patients who underwent distal gastrectomy were divided into 3 groups based on the anastomosis type: Billroth-I, Billroth-II, or Roux-en-Y.
Laboratory assays
The nutritional statuses of the gastric cancer patients were assessed before and 1–5 years after surgery, using measured body weights, total lymphocyte counts (TLCs), and serum hemoglobin, total protein, albumin, cholesterol, and transferrin levels. Anemia was defined according to the World Health Organization (WHO) criteria as an hemoglobin level <12 g/dL for women, or <13 g/dL for men [13].
Nutritional risk index (NRI) and prognostic nutritional index (PNI)
NRI was calculated using the following formula:
Although the “usual” weight is generally defined as the stable weight ≥6 months before the illness, this value was not routinely determined for our patients. Therefore, the weight measured at admission for surgery was used as the “usual” weight. Patients were deemed to be malnourished when the NRI score was <97.5 [14].
Statistical analysis
For subjects whose body weight data were missing from the medical records, we applied multiple imputations (MIs; 5 imputations) using the MI procedure in the Statistical Analysis System (SAS Institute, Cary, NC, USA) [15]. Continuous values are expressed as means with standard deviations. The mean values of the 2 patient groups were compared using 2-tailed t-tests, and the mean values of 3 patient groups were compared using analysis of variance (ANOVA). Post-hoc comparisons were made using the Bonferroni method. P-values ≤0.05 were generally considered to indicate statistically significant differences. However, to avoid a type I error in post-hoc analyses, a P-value of 0.05/3 (0.017) was set as the threshold for statistical significance. All statistical analyses were performed using SPSS version 21.0 software (IBM SPSS Inc., Chicago, IL, USA).
Human rights and informed consent statements
All procedures were followed in accordance with the ethical standards of the responsible committees on human experimentation (institutional and national), as well as the Helsinki Declaration of 1964 and later versions. Informed consent, or a valid substitute, was obtained from all patients prior to inclusion in the study.
RESULTS
Clinicopathological patient characteristics
During the study period, 821 patients underwent curative gastrectomy for gastric cancer. Of these, 163 were excluded because they died (n=51), were lost to follow-up (n=28), or developed a recurrence (n=84) within 5 years postoperatively. Accordingly, 658 patients formed the study population.
The study cohort included 422 (64.1%) and 236 (35.9%) male and female patients, respectively, with a mean age at diagnosis of 58.3 years (range, 20–83 years) (Table 1). Within the cohort, 118 (17.9%) and 540 (82.1%) did and did not undergo chemotherapy, respectively, and 89 (13.5%) and 569 (86.5%) underwent total and distal gastrectomy, respectively. Of the 565 patients who underwent distal gastrectomy, 403 (70.8%), 112 (19.7%), and 54 (9.5%) underwent Billroth-I, Billroth-II, and Roux-en-Y anastomosis, respectively.
Table 1
Characteristics of 658 patients who underwent curative resection during the study period

Comparison of the patients who underwent total and distal gastrectomy
Table 2 shows the NRI, body mass index (BMI), PNI, and laboratory values of patients who underwent total and distal gastrectomy before and 1–5 years after surgery. Before surgery, the 2 groups did not differ significantly in terms of any variable. However, 1–5 years after surgery, the total gastrectomy group had significantly lower NRI, BMI, and hemoglobin levels and significantly higher TLCs, compared with the distal gastrectomy group. The former group also had significantly lower serum albumin and cholesterol levels and significantly higher total protein levels relative to the latter group 1–4 years after surgery; however, by the fifth year, these differences were no longer observed. The total gastrectomy group also developed significantly higher transferrin levels, starting 3 years after surgery. The 2 groups never differed in terms of PNI.
Table 2
Comparison of the laboratory values of patients who underwent distal or total gastrectomy, measured before, and 1–5 years after, curative resection

Data are shown as means±standard deviations. Institutional reference values: TLC, 2,000–4,400 ×106/L; hemoglobin, 13–17 g/dL; serum albumin, 3.3–5.2 g/dL; total protein, 6–8 mg/dL; cholesterol, 0–200 mg/dL; transferrin, 250–380 mg/dL. NRI was calculated using the following formula: 1.519×serum albumin (g/L)+0.417×(present weight/usual weight×100); PNI was calculated using the following formula: 10×serum albumin value (g/dL)+0.005×TLC in the peripheral blood (per mm3).
NRI = nutritional risk index; NA = not applicable; BMI = body mass index; PNI = prognostic nutritional index; TLC = total lymphocyte count.
*A statistically significant difference compared with patients who underwent chemotherapy (P<0.05), as determined by an independent t-test.
An analysis of the incidence of anemia showed that at all time points after surgery, but not before surgery, patients who underwent total gastrectomy were significantly more likely to have anemia than were those who underwent distal gastrectomy (Fig. 1A). The total gastrectomy group exhibited a sharp increase in the anemia incidence from 27% before surgery to 51.8% 1 year after surgery, followed by a decrease 40.7% at year 2 and subsequent increase to 55.1% at year 5. By contrast, the anemia rates in the distal gastrectomy group only increased slightly over time from 20.1% before surgery to 28.1% at year 5.
Fig. 1
Incidence of anemia and malnutrition 1–5 years postoperatively among patients who underwent total or distal gastrectomy (A and B) or did or did not undergo chemotherapy (C and D). Anemia was defined as a hemoglobin levels <12 g/dL for women or <13 g/dL for men. Malnutrition was defined as a NRI of <97.5. NRI was calculated using the following formula: 1.519×serum albumin (g/L)+0.417×(present weight/usual weight×100).
Preop. = preoperative; NRI = nutritional risk index.
*P<0.05, as determined by the χ2 test.
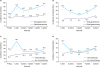
An analysis of the incidence of malnourishment showed that patients who underwent chemotherapy were significantly more likely to be malnourished compared to those who did not, at all postoperative time points except during year 3.
Comparison of patients who did and did not undergo chemotherapy
Table 3 shows the NRI, BMI, PNI, and laboratory values of the chemotherapy and non-chemotherapy groups 1–5 years after curative gastrectomy. Before surgery, patients who underwent chemotherapy had a significantly lower PNI, compared to patients who did not, and this difference was maintained for 1 year after surgery. Thereafter, the 2 groups had equivalent PNI values. This pattern was also observed for serum hemoglobin, albumin, and cholesterol levels. The total protein levels exhibited a similar pattern, except that the chemotherapy group also had lower total protein levels 2 years after surgery. The 2 groups did not differ in terms of BMI at any time point. The NRI and TLCs were only lower in the chemotherapy group 1 year after surgery.
Table 3
Comparison of the laboratory values of patients who did and did not undergo chemotherapy, measured before, and 1–5 years after, curative resection

Data are shown as means±standard deviations. Institutional reference values: TLC, 2,000–4,400 ×106/L; hemoglobin, 13–17 g/dL; serum albumin, 3.3–5.2 g/dL; total protein, 6–8 mg/dL; cholesterol, 0–200 mg/dL; transferrin, 250–380 mg/dL. NRI was calculated using the following formula: 1.519×serum albumin (g/L)+0.417×(present weight/usual weight×100); PNI was calculated using the following formula: 10×serum albumin value (g/dL)+0.005×TLC in the peripheral blood (per mm3).
NRI = nutritional risk index; NA = not applicable; BMI = body mass index; PNI = prognostic nutritional index; TLC = total lymphocyte count.
*A statistically significant difference compared with patients who underwent chemotherapy (P<0.05), as determined by an independent t-test.
An analysis of the incidence of anemia per the above definition found that the chemotherapy and no-chemotherapy groups did not differ significantly in terms of the anemia incidence before surgery. However, 1 year after surgery, the chemotherapy group exhibited a sharp increase in anemia from 33.1% (before surgery) to 62.1%. Thereafter, anemia rates dipped to 30.6% at year 2, followed by an increase to 36.8% at year 5 (Fig. 1B). By contrast, the anemia rates in the chemotherapy group only increased slightly, from 18.4% before surgery to 30.9% at year 5. The 2 groups differed significantly at year 1.
An analysis of the incidence of malnutrition, defined as a NRI <97.5, found that chemotherapy patients were significantly more likely to be malnourished 1 year after surgery, compared to the no-chemotherapy patients (20.7% vs. 8.8%) (Fig. 1C). At year 2, the malnutrition rate of the chemotherapy group decreased by half to 11.9%, and the rate of the no-chemotherapy group increased to 11.2%. Thereafter, the 2 groups maintained similar rates and slight increases over time to 15.1% and 14.7% at year 5, respectively.
Comparison of patients who underwent Billroth-I, Billroth-II, and Roux-en-Y anastomosis after distal gastrectomy
The 3 anastomosis groups did not differ in terms of NRI, PNI, BMI, TLCs, and serum albumin levels preoperatively or during the 5-year follow-up period (data not shown). Table 4 lists the total protein, cholesterol, and transferrin values of the Billroth-I, Billroth-II, and Roux-en-Y groups before and 1–5 years after curative gastrectomy. An ANOVA, followed by a Bonferroni post-hoc analysis, showed that preoperatively, the 3 groups did not differ significantly in terms of total protein, cholesterol, and transferrin values. After surgery, the Billroth-I group had significantly higher total protein levels than the Billroth-II group at all time points, as well as higher cholesterol levels at years 1 and 4, and significantly lower transferrin levels at year 5.
Table 4
Comparison of the laboratory values of patients who underwent Billroth-I, Billroth-II, or Roux-en-Y anastomosis, measured before, and 1–5 years after, distal gastrectomy

DISCUSSION
This study measured the nutritional statuses, including BMI, laboratory values, and the nutritional evaluation tools such as NRI and PNI [14161718], of patients for 5 years after radical treatment for gastric cancer. The NRI was designed to predict surgery-related complications in malnourished patients. As this index correlates with malnutrition [19], it has been used to assess the nutritional statuses of patients with head and neck [2021] and gastrointestinal cancers [161722]. Although the NRI is based on a simple calculation, it is a useful nutritional status screening tool because it employs objective variables (body weight and serum albumin levels) that are important indicators of malnutrition [232425]. The present study showed that the total gastrectomy group had significantly lower NRI values 1–5 years after surgery. Similarly, the total gastrectomy group had significantly higher malnutrition rates (NRI <97.5%) than did the distal gastrectomy group at all time points after surgery, except year 3. Therefore, although patients who undergo total gastrectomy do adapt somewhat after surgery, the operation is associated with a poorer long-term nutritional status. Accordingly, these patients should be monitored closely and given appropriate nutritional support for at least 5 years after surgery.
The present study also showed that patients who underwent chemotherapy had significantly lower NRI values and malnutrition rates 1 year after surgery, than those treated with gastrectomy alone. Therefore, the nutritional statuses of patients who undergo chemotherapy should also be monitored closely to ensure appropriate nutritional support for at least 1 postoperative year.
The PNI reflects the prognosis of curative gastrectomy [2627]. The early detection of recurrences and continuation of effective chemotherapy are critical for prolonging the long-term survival of patients with gastric cancer who undergo curative gastrectomy; similarly, supportive treatments such as nutritional therapy might also assist gastric cancer patients with low PNI values. However, in the present study, only the chemotherapy group had significantly lower PNI values both before and 1 year after surgery, compared with the no-chemotherapy group. By contrast, the total and distal gastrectomy groups did not differ in terms of PNI at any time point. This finding reflects the fact that all study patients lacked evidence of recurrence. Accordingly, in the absence of recurrence, PNI is more effective for predicting outcomes than for determining the nutritional status. We therefore assume that PNI does not directly reflect the nutritional status.
The present study found that the total gastrectomy group had a significantly higher TLC and plasma transferrin level, compared with the distal gastrectomy group. Various studies have yielded conflicting results regarding the ability of the TLC to reflect the nutritional status [2829]. In our study, however, the TLC was not a suitable marker of malnutrition relative to the extent of gastrectomy. We note that elements such as aging and chemotherapy can affect the results, and that many factors should be considered when determining whether the TLC reflects the nutritional status.
Transferrin is an iron-binding blood plasma glycoprotein that controls free iron levels in biological fluids [30]. Increased plasma transferrin levels are often seen in patients with iron deficiency-related anemia [31]. Indeed, an analysis of the anemia incidence in the total and distal gastrectomy groups showed that whereas the 2 groups had similar rates of anemia before surgery, total gastrectomy was associated with a significant postoperative increase in anemia that was maintained for 5 years. This finding suggests that total gastrectomy patients should be monitored for anemia for at least 5 postoperative years and appropriate interventions should be applied, if necessary.
The chemotherapy group experienced a similar sharp increase in the anemia incidence 1 year after surgery, followed by a decrease to the incidence observed in the no-chemotherapy group. Therefore, patients who undergo chemotherapy should be carefully monitored for anemia for at least 1 year after surgery.
Regarding distal gastrectomy, the present study did not find that the type of anastomosis affected the postoperative nutritional status. However, we did find that Billroth-I anastomosis was associated with higher cholesterol levels after surgery, compared with Billroth-II anastomosis.
To the best of our knowledge, our study was the first to examine the nutritional statuses of gastric cancer patients who underwent curative gastrectomy and did not develop recurrences within 5 years after surgery. We determined that patients who undergo total gastrectomy should be monitored for malnutrition and anemia for at least 5 years after surgery, whereas the patients who undergo chemotherapy should be monitored for malnutrition and anemia for at least 1 year after surgery. Such monitoring will likely improve the quality of life of those who undergo curative gastrectomy. However, this study was limited by its reliance on retrospective data, which could have introduced information bias. In addition, this was a single-center study, and may therefore have been prone to selection bias. Prospective large-scale studies that examine nutritional statuses during long postoperative periods and use more objective tools, such as subjective global assessment [32] and nutritional risk screening (NRS 2002) [33], are warranted.
 XML Download
XML Download