

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since the introduction of laparoscopic distal gastrectomy (LDG) in 1994 by Kitano et al. [1], this method has been extensively used to treat patients with distal gastric cancer (GC). However, despite the well-known benefits of laparoscopic over open gastrectomy, totally laparoscopic total gastrectomy (TLTG) is a procedure less often performed due to its technical difficulty. Specifically, laparoscopic esophagojejunostomy (EJ) is one of the most critical steps during TLTG. In fact, multiple EJ reconstruction methods have been described and none is considered a standard technique [2].
In our initial experience with laparoscopic gastrectomy at our 2 affiliated teaching hospitals, the EJ leak rates were 6% and 8%, respectively [34]. After these initial results using a single-layer hand-sewn EJ anastomosis, we decided to modify and develop a new EJ reconstruction technique.
The present study aimed to describe a 2-layer hand-sewn EJ technique during TLTG and evaluate postoperative morbidity.
MATERIALS AND METHODS
This retrospective cohort study included all consecutive patients who underwent TLTG for GC from 2012 to 2016 at our 2 affiliated teaching hospitals.
We assessed epidemiological and perioperative data. Patients were stratified according to the American Society of Anesthesiologists physical status classification.
The preoperative evaluation included an upper gastrointestinal endoscopy, biopsy, complete blood count, liver function tests, electrocardiogram, and nutritional evaluation. Preoperative imaging included thorax-abdomen-pelvis computed tomography (CT). The selection of cases for laparoscopic total gastrectomy included patients with clinical early gastric cancer (EGC) who were not candidates for endoscopic resection and patients with advanced gastric cancer (AGC) without clinical invasion of the esophagus or adjacent structures, such as the pancreas or liver, and with lymph node metastases only in the perigastric area. All surgeries where performed by attending surgeons experienced in laparoscopic surgery for benign gastric pathology and GC.
Surgical technique
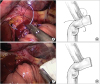
Our TLTG technique has been previously described [34]. A pneumoperitoneum with CO2 at 15 mmHg is established. Six laparoscopic ports and a 30°-scope are utilized, with a subxiphoid 5-mm port for the liver retractor (Fig. 1). All major vessels (right and left gastroepiploic and right and left gastric vessels) are identified and double-clipped. The duodenum is divided using a 60-mm linear stapler. Lymph node dissection is performed according to the Japanese guidelines [5]. The esophagus is divided using a 60-mm linear stapler. We did not perform a routine frozen section for proximal resection margin because these were selected patients without esophageal invasion. The surgical specimen is extracted through a suprapubic incision because of large specimen size in AGC and fatty omentum generally present in our patient population (Fig. 1).

A jejunal loop, 30 cm from the ligament of Treitz is transected with a linear stapler and a Roux-en-Y reconstruction is performed. A retrocolic route is preferentially utilized. All participating surgeons performed a standardized intracorporeal 2-layer hand-sewn EJ. The steps of the EJ anastomosis are demonstrated in Figs. 2, 3, 4 (see also Supplementary Video Clip). To minimize esophageal retraction into the mediastinum after esophageal transection, a 34-38-Fr blunt bougie is advanced through the mouth down to the esophageal distal end; this helps to maintain the esophagus in the abdominal cavity during the EJ, especially in the first posterior layer. The anastomosis starts by suturing the jejunum to the distal end of the esophagus under the staple line with an absorbable 3.0 suture (Vicryl®; Ethicon, Somerville, NJ, USA). Afterwards, the anterior esophageal wall is opened immediately above the stapler line and an enterotomy is also created in the anterior aspect of the jejunum. Next, a second posterior layer and the first anterior layer of the EJ are formed with a running 3.0 absorbable suture (Vicryl®). The bougie is advanced through the anastomosis. A second anterior seromuscular layer is formed with a running 3.0 absorbable monofilament suture (Monocryl® or PDS®; Ethicon). It is important to avoid a complete esophagotomy, especially on the right side, to minimize difficulty in suturing the mucosa in this area. It is also important to have the assistant grasp the suture material gently as the anastomosis is performed. Finally, a methylene blue test is performed to rule out a leak. The jejunojejunostomy is performed intracorporeally with a linear stapler. Two drains are placed at the end of the surgery.
Fig. 2
Two-layer hand-sewn EJ. First posterior layer: a 34-Fr bougie is placed inside the esophagus (A). Suturing the jejunum to the distal end of the esophagus under the complete staple line (B-D).
EJ = esophagojejunostomy.

Fig. 3
Two-layer hand-sewn EJ. The second posterior layer and the first anterior layer: the anterior esophageal wall is opened immediately above the stapler line and an enterotomy is also created in the jejunum (A). A second posterior layer (B-D) and the first anterior layer are formed (E, F).
EJ = esophagojejunostomy.

Fig. 4
Two-layer hand-sewn EJ. A second anterior layer is formed (A, B) and the anastomosis is completed (C, D).
EJ = esophagojejunostomy.
An oral contrast study is performed on postoperative day 3–5. After this study, the patient starts an oral diet and prophylactic drains are removed. The patients are discharged when they are able to tolerate a soft diet for 24 hours. Patients are routinely scheduled to undergo upper endoscopy 3 months after surgery, or sooner if symptoms of stenosis appear.
We consider EJ leak as the appearance of contrast outside the anastomosis in an oral contrast study or on CT or by direct evaluation at reoperation. We consider EJ stenosis as the inability to advance a standard gastroscope through the anastomosis or the need for endoscopic dilation. Complications are evaluated according to the Clavien-Dindo classification, and a Clavien score 3 or higher is considered a major complication [6]. Staging is based on the tumor, node, and metastasis (TNM) American Joint Committee on Cancer (AJCC) 7th edition [7]. Continuous variables were described by means and standard deviations or medians and ranges. Categorical variables were described with frequencies and percentages. The ethics committee approved this study.
Ethics statement
All procedures were followed in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent or an equivalent was obtained from all patients included in the study.
RESULTS
We included 51 patients who underwent TLTG for GC and a standardized EJ. Twenty-seven (53%) were male, the median age was 60 (36–87) years, and the median body mass index (BMI) was 25 (19–32). Twenty-three (45%) patients had a previous laparotomy and 38 (74%) had at least one comorbidity (Table 1). The location of the tumor was in the upper two-thirds of the stomach in 42 (82%) patients.
Table 1
Epidemiological patient data for a TLTG and EJ

The average operative time was 337±71 minutes and the intraoperative bleeding was 160±107 mL. There were no conversions related to EJ (Table 2).
Table 2
Clinical outcome data for a TLTG and EJ

Postoperative morbidity was observed in 9 (17%) patients (Table 2). There was no postoperative mortality and only one patient required reoperation due to duodenal stump leak. This was the only major complication and was not related to the EJ. Leakage from EJ was observed in 2 patients (3.8%). Both patients were successfully and conservatively managed with restriction of oral intake and total parenteral nutrition. The duration of hospitalization in these 2 patients was 28 and 29 days, respectively, and both were discharged when there was no evidence of persistent EJ fistula, a soft diet was tolerated, and the remaining drains were removed. One patient (1.9%) required endoscopic dilation due to EJ stenosis. The median length of hospital stay was 8 (6–29) days. There were no readmissions, and one patient was treated with oral antibiotics due to a small periduodenal collection 3 weeks after surgery.
Tumor pathology was EGC in 27 (53%) and AGC in 24 (47%) patients. All patients without distant metastasis had an R0 resection without positive margin on the esophagus, and only 1 patient had a palliative gastrectomy because he presented with multiple liver metastases. The median tumor size was 3.0 cm (range 0.3–11.0 cm). The median lymph node count was 40 (10–103) in patients with curative surgery, and 97% of patients had a lymph node count over 15. Lymph node metastases were present in 17 (33%) patients. The distribution of patients in stages I, II, III, and IV was 56%, 19%, 21%, and 1%, respectively (Table 3).

DISCUSSION
Randomized controlled trials and meta-analyses have confirmed better postoperative outcomes with laparoscopic gastrectomy compared to open surgery, including less intraoperative blood loss, less postoperative pain, a shorter hospital stay, and decreased morbidity, with comparable oncological results [8910]. Despite the postoperative benefits of laparoscopic gastrectomy, fewer TLTG cases are performed than LDG cases, mainly due to the technical difficulty of laparoscopic EJ and the risk of complications associated with EJ leak.
There are several factors that make EJ anastomosis a complex step in TLTG. This anastomosis is performed high in the abdomen at the level of the narrow diaphragmatic crura, where adequate triangulation in some cases can be challenging. In addition, the esophagus naturally retracts into the mediastinum after transection. Finally, some patient characteristics, such as central obesity and presence of hiatal hernia, which are commonly present at the time of surgery in patients with proximal tumors, can add further difficulty.
To overcome some of these challenges, we designed this method of EJ based on a similar anastomosis regularly performed at our center for gastrojejunostomy in laparoscopic Roux-en-Y gastric bypass; we have experienced over 2,500 such cases with a leak rate under 1% [11]. Few reports have previously described laparoscopic hand-sewn EJ, but there are no publications with a significant number of cases describing postoperative results [12].
A variety of techniques have been described to perform EJ after TLTG. To avoid the limitations of the minimally-invasive approach, some groups have used extracorporeal EJ through a small upper laparotomy [1314]. However, sometimes it is necessary to increase the length of the incision to obtain a better view of the anastomosis, especially in overweight patients, and thus some of the benefits of minimally-invasive surgery are potentially lost. Our study population had a BMI of 25, and for this reason, we have not pursued this technique.
The use of linear staplers for EJ has been reported [1516]. This technique requires extensive dissection of the distal esophagus and crura, which might increase the risk of bleeding and further development of hiatal hernia. From a technical point of view, a latero-lateral EJ using a linear stapler can increase the tension on the upper portion of the anastomosis and thus increase the risk of a more difficult to treat leakage into the mediastinum. The EJ we describe requires less dissection of the crura and distal esophagus and allows the placement of the EJ at the level of or below the crura, which makes a potential leak easier to manage and avoids injury to the thoracic structures during EJ.
Another type of EJ has been described using a circular stapler, which mimicked the most commonly performed open EJ [1718]. However, this technique has some limitations compared to our hand-sewn EJ. It requires an increase in the size of one of the laparoscopic ports to accommodate and introduce the stapler, and there is a potential risk of jejunal limb rotation or twisting.
A variation in this technique allows the surgeon to perform the EJ without the need of a purse-string suture at the end of the esophagus. In this technique, a transoral anvil insertion potentially facilitates the EJ and reduces the operative time [219]. However, a shortcoming of this technique is the overlap between the linear and circular stapler lines, which could increase the risk of leakage; moreover, the anvil must be passed through the pharynx and the full length of the esophagus, making it potentially difficult to diagnose injury to these organs. There is a higher cost involved with this type of circular stapler, as well as a concern about abdominal contamination with the nasogastric tube passing through the esophagus to the peritoneal cavity.
At our 2 hospitals, the use of a single-layer hand-sewn EJ showed leak rates of 6% and 8%, respectively [34]. The results obtained with the 2-layer hand-sewn EJ described in this paper are better than our historical data, as this method reduced EJ leak rates to 3%, and EJ stenosis to 1%. Some of this improvement may be due to a learning-curve effect, but we believe that adding a double layer to the anastomosis and using a bougie to maintain the esophagus in the abdominal cavity during the EJ are at least in part responsible for this improved result. Laparoscopic EJ series in over 50 patients describe EJ a leak rate as low as 1.5% and as high as 4.8%, and an EJ stenosis rate between 0% and 9% [2]. Our method is not superior or inferior to these results but is comparable, and provides an alternative for alimentary tract reconstruction after TLTG. Several EJ methods have proven to be safe and feasible [131516171819]. However, comparisons of different EJ techniques are difficult due to the lack of comparative trials and the low rate of EJ leak [20]. The best method of laparoscopic EJ should be determined in a randomized controlled trial; however, it is unlikely that such a study will be performed in the near future.
The potential benefits of our EJ method are the following: it avoids a laparotomy and unnecessary dissection on the distal esophagus and lower mediastinum, and there is no extension of port incisions to introduce stapling devices or need to pass the anvil through the pharynx and esophagus. In the case of EJ leak, it is unlikely that mediastinitis will develop due to the intra-abdominal position of the anastomosis; supporting this argument, both of our patients who developed a leak were managed with prophylactic drains. Finally, the costs of this EJ are potentially lower because no stapling device is used in this part of the procedure.
A major limitation of this technique is that it requires advanced minimally-invasive intracorporeal knotting and suturing skills. However, this limitation can be successfully overcome with adequate laparoscopic training models and previous experience in less technically demanding gastrointestinal anastomoses [1121]. Another limitation of our study is the still relatively low number of cases than for open EJ and the lack of a control group.
In conclusion, 2-layer hand-sewn EJ during TLTG for GC is feasible and safe. This method avoids a laparotomy for reconstruction and the disadvantages associated with the laparoscopic introduction of mechanical staplers for EJ, and provides an alternative for alimentary tract reconstruction after TLTG.
 XML Download
XML Download