

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Despite the decreasing incidence and mortality from gastric cancer, this entity remains a major health problem worldwide. Gastric cancer is the fourth most common malignancy and the second leading cause of death due to cancer. About 90% of gastric cancers are adenocarcinomas. Many risk factors, such as Helicobacter pylori infection, obesity, gastro-esophageal reflux disease, cigarette smoking, and dietary factors, are implicated in the development of this type of cancer. Other less common factors include pernicious anemia, Epstein-Barr virus infection, radiation, prior gastric surgery for benign conditions, blood type A, and some hereditary syndromes. Here, we report a case of metachronous gastric adenocarcinoma, which developed seven years after successful treatment of the primary gastric diffuse large B-cell lymphoma (DLBCL).
CASE REPORT
We report the case of a 73-year-old man who presented with epigastric pain and weight loss in February 2007. No abnormalities were found on physical examination. Contrast-enhanced abdominal computed tomography (CT) scan revealed a 3-cm circumferential gastric wall thickening mainly marked at the fundus and antrum, without contrast enhancement (Fig. 1). Gastric endoscopy showed a congestive and edematous antral mucosa. Biopsies confirmed the diagnosis of malignant DLBCL, and H. pylori infection was detected (Fig. 2). Immunohistochemical analysis revealed most cells to be CD20 positive (Fig. 3). Staging was completed by performing cervical, thoracic, and pelvic CT scans, and the disease was classified as stage I–E according to the Ann Arbor classification system. Adequate therapy comprising proton pump inhibitors and antibiotics was administered to treat the H. pylori infection. Immunochemotherapy was started according to clinical guidelines. The patient received six courses of R-CHOP (cyclophosphamide, adriamycin, vincristine, prednisolone plus rituximab). Four prophylactic intrathecal injections of methotrexate were administered. The patient's treatment ended in July 2007 without major complications. Follow-up endoscopy and imaging (Fig. 4) performed three months later showed complete remission; however, the H. pylori infection persisted despite administering adequate first-line antibiotic treatment. Second-line antibiotic treatment was initiated, and the patient was advised to make follow-up visits to the gastroenterology outpatient clinic.
Fig. 1
Abdominal computed tomography scan: 3-cm circumferential wall thickening of the entire stomach, mainly at the fundus and antrum, can be seen. Absence of contrast enhancement.
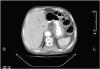
Fig. 2
Diffuse interstitial infiltration by large lymphoid cells, CD20+, CD10−, and cyclin D1 (H&E, ×100).

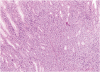
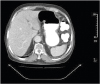
Fig. 4
Computed tomography scan of the abdomen 4 months after completion of chemotherapy showing complete resolution of the previously noted gastric tumor.
The patient did not make follow-up visits, but presented to our facility in October 2014 with recurrent epigastric pain along with progressive weight loss. Gastroscopy revealed the presence of ulcerative lesions, indicative of malignancy localized at the fundus. Biopsy confirmed the presence of microfoci of invasive adenocarcinoma of the intestinal type with lymphatic permeation (Fig. 5). Immunohistochemical analysis revealed positive anti-c-erbB2 (score 3+). H. pylori infection was also detected. Initial staging performed with cervical, thoraco-abdominal, and pelvic CT scans showed diffuse peritoneal carcinomatosis without hepatic involvement. Staging laparoscopy was not performed.
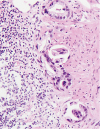
Fig. 5
Glandular proliferation lined with cylindrical epithelial cells with atypical and hyperchromatic nuclei that are compatible with microfoci of invasive gastric adenocarcinoma of the intestinal type (H&E, ×400).
Platinum-based chemotherapy was started along with anti-human epidermal growth factor receptor 2 targeted therapy (cisplatin, 5-fluorouracil, trastuzumab). Ten days after the third cycle, the patient was emergently admitted for septic shock, rapid deterioration, and multi-organ failure leading to death.
DISCUSSION
In the era of new targeted therapies, the overall survival rate of patients with non-Hodgkin lymphomas has improved; however, there is an increase in the rate of secondary malignancies in survivors. While acute leukemia is the most common secondary malignancy, solid tumors, especially carcinomas, are also common [1].
Primary gastric lymphoma is one of the most common extra-nodal lymphomas and represents 5% to 10% of all gastric malignancies [23]. Although cases of metachronous gastric adenocarcinoma after primary gastric lymphoma have been described in the literature, it is a very uncommon entity. It has a higher malignant potential as compared to sporadic cases [45]. Many studies have reported a six-fold increase in the incidence of gastric carcinoma in patients treated for gastric lymphoma of mucosa-associated lymphoid tissue as compared to in the general population [25]. The incidence of metachronous gastric adenocarcinoma after gastric lymphoma is 12% according to a retrospective study published by Inaba et al. [5]. The median time from the diagnosis of gastric lymphoma to gastric adenocarcinoma is 3.5 to 34 years [5].
In fact, most patients with metachronous gastric cancer after primary gastric lymphoma are diagnosed in the advanced stages. This is mainly due to a prolonged pre-diagnostic interval during which patients may not undergo regular follow-up tests [6]. Most patients die within 18 months of diagnosis [6]. However, Nakamura et al. [3] did not report a survival rate in their study.
Many risk factors are implicated, of which H. pylori infection is the most important. Untreated chronic H. pylori infection can lead to the development of chronic gastritis, chronic atrophic gastritis, intestinal metaplasia, and gastric adenocarcinoma [25]. At present, it is still unclear whether treatment of H. pylori infection will prevent the development of gastric cancer as the available data are controversial. In a randomized control trial, Leung et al. [7] showed that eradication of the infection prevented the transformation of premalignant gastric lesions into gastric cancer in 52.9% of the cases. In contrast, in China, Wong et al. [8] showed that the incidence of gastric cancer was similar between patients in whom the infection had been treated and those in whom the infection remained untreated.
Other causes include previous gastric surgery, which results in prolonged exposure of the remaining mucosa to alkaline secretion (bile salts reflux) [4
910]. Gastroesophageal reflux, adenomatous polyps, and formation of carcinogenic nitrosamines when the gastric pH drops below 5.5 are also involved in the pathophysiology of secondary gastric carcinomas [10]. Inaba et al. [5] also demonstrated, although the significance was marginal (P=0.070), that the incidence of metachronous gastric carcinoma was higher in older populations (age, >60 years), in patients with stage II–IV disease (according to the Ann Arbor classification), in DLBCL subtype and in patients who received chemotherapy [1]. Many drugs are known to have mutagenic and carcinogenic effects [4]. Of these, alkylating agents and topoisomerase II inhibitors are the two families that have been identified by the World Health Organization [11]. These drugs are associated with an increased incidence of hematological malignancies. Further, radiation therapy can induce solid tumors, typically within the radiation field, at doses above 45 Gy [12]. Solid tumors are usually diagnosed 14 to 26 years after radiation therapy [13].
Most patients were treated according to the disease stage, as per conventional guidelines for the treatment of primary gastric adenocarcinomas. In Japan, owing to the increased frequency of follow-ups, the disease is commonly detected in the early stages. A conservative approach, such as endoscopic mucosal resection, is therefore adopted, with more advanced cases being treated with surgery, when indicated, or palliative chemotherapy [1]. Cisplatin, 5-fluorouracil, and mitomycin C regimens in various combinations are commonly used [1].
There are two theories that could explain how the risk factors contribute to an increased risk of secondary gastric carcinoma following primary gastric lymphoma. The first theory is that the different causative factors (H. pylori infection, chemotherapy, radiation, etc.) damage the gastric mucosa. The second theory is that the carcinoma was probably too small to be detected at the time of the gastric lymphoma diagnosis [4514]. Patients in whom the interval between the development of the two tumors was short might have had a carcinoma that went undetected at the time of the first diagnosis. Whereas, patients in whom the interval was longer would have developed the carcinoma secondary to accumulating risk factors and treatment [3].
The case described in this report has many common elements. Our patient was an elderly man with primary gastric DLBCL, and complete remission was achieved after treatment with an alkylating agent-based chemotherapy regimen (R-CHOP). H. pylori infection remained active despite administering adequate combined treatment with proton pump inhibitors and antibiotics, which contributed to sustained chronic gastritis. The mean time to diagnose the metachronous gastric carcinoma was seven years, which is similar to what is described in the literature (3.5 to 34 years). In the present case, five of the major risk factors were present. We believe that a combination of many carcinogenic-related risk factors, of which chronic H. pylori infection was the most important, led to the development of gastric carcinoma following primary gastric lymphoma.
In summary, patients who have achieved complete remission after receiving treatment for primary gastric lymphoma should be followed-up at regular short intervals. Further, H. pylori infection should be diagnosed promptly and treated aggressively. Clinicians should educate their patients about the possible development of secondary gastric cancer, which can be fatal.
 XML Download
XML Download