

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The proportion of early gastric cancer (EGC) cases has increased among surgically treated patients with gastric cancer in Eastern Asia and some Western countries. As the incidence of EGC has increased, minimally invasive surgeries have been performed more widely [1].
Among minimally invasive surgery techniques, pylorus-preserving gastrectomy (PPG) is an attractive option for the treatment of EGC to reduce the development of dumping syndrome and postoperative malnutrition [2]. However, PPG can cause delayed gastric emptying with early fullness and vomiting associated with pyloric spasm. The reported incidence of delayed gastric emptying after PPG ranges from 6.2% to 8.0% [34]. The reasons for delayed gastric emptying are not well-established. In a study of resection of the pyloric branch of the canine vagus nerve, gastric stasis developed during the early postoperative period, caused by tonic and phasic contractions of the pylorus [5].
Botulinum toxin has been found to be effective in the treatment of spastic disorders of the smooth muscle. In light of this observation, botulinum toxin could interfere with the tonic contraction of the pylorus, which may be the reason for the improvement of gastric stasis after botulinum toxin injection. It has already been used for the prevention and treatment of gastric stasis as a complication of esophagectomy associated with vagotomies [6], diffuse esophageal spasm, achalasia, and refractory gastroparesis [6789]. However, no report has evaluated intrapyloric botulinum toxin injection for the treatment of patients with delayed gastric emptying after PPG.
Here, we describe our experience in using intrapyloric botulinum toxin injection to manage patients who complain of gastric stasis symptoms after PPG.
MATERIALS AND METHODS
From February 2012 to July 2015, 177 patients with EGC underwent laparoscopic-assisted or robotic-assisted PPG at the National Cancer Center of Korea. A total of 13 patients (7.3%) needed managements for delayed gastric emptying after surgery. Seven of these recovered with conservative treatment, such as Levin tube insertion and prokinetics. The other 6 patients were treated with botulinum toxin injection. Informed consent was obtained from all the patients before the procedure. This study conforms to the ethical standards of the Institutional Review Board of the National Cancer Center, Korea and the Helsinki Declaration of 1964 and later versions. Thus, this study was approved by the Ethics Review Board of the National Cancer Center (study number: NCC2016-0177).
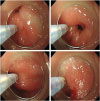
Botulinum toxin (25–50 IU per injection; total, 100–200 IU in 5 mL of 0.9% normal saline solution) was injected into the 4 quadrants of the prepyloric area (within 1 cm of the pyloric channel) after the sclerotherapy needle tip was buried firmly into the gastric wall. These procedures were performed by 3 expert endoscopists (Fig. 1).
Fig. 1
Endoscopic botulinum toxin injection into the pylorus area. Botulinum toxin (25−50 IU per site; total, 100−200 IU) is injected into each quadrant of the pylorus area using a standard sclerotherapy needle via capped endoscopy.
We retrospectively reviewed the outcome of this procedure using medical records and telephone interviews. The Gastric Outlet Obstruction Scoring System (GOOSS) was used to assess the severity of symptoms before and after botulinum toxin injection as follows: 0) no oral intake; 1) only liquid diet; 2) soft solid diet; and 3) low residue or full diet [1011]. We checked the GOOSS score of each patient before and 10 days after the procedure and at every outpatient clinic visit. Improvements in delayed gastric emptying were defined as the relief of gastric outlet obstruction symptoms or improvement in the GOOSS score 10 days after the procedure.
We also evaluated the improvements in delayed gastric emptying using endoscopic criteria. The amount of residual food was classified into 4 grades: grade 0, no residual food; grade 1, a small amount of residual food; grade 2, a moderate amount of residual food, but possible to observe the entire surface of the remnant stomach with body rolling; and grade 3, a large amount of residual food that hinders observation of the entire surface even with body rolling [12].
RESULTS
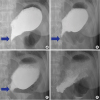
All patients' detailed clinical characteristics are shown in Table 1. Five patients who received botulinum toxin injection showed symptom improvements, particularly in tolerating soft solid or full diet within 10 days, i.e., the GOOSS score improved from 0 to 2 or 3 (Table 2). Upper gastrointestinal series and subsequent daily simple abdominal X-rays showed that pyloric spasm had improved, and gastric emptying was resolved (Fig. 2). One patient improved, i.e., able to ingest a soft fluid diet within 10 days, and was discharged. We confirmed the further improvement of his diet to a soft solid diet at the outpatient clinic 1 month after botulinum toxin injection.
Table 1
Clinical characteristics of the post-PPG patients who underwent intrapyloric botulinum toxin injection

PPG = pylorus-preserving gastrectomy; BMI = body mass index; TNM = tumor, node, and metastasis; LN = lymph node; F = female; M = male; LAPPG = laparoscopic-assisted pylorus-preserving gastrectomy; RAPPG = robotic-assisted pylorus-preserving gastrectomy; LB = lower body; GC = greater curvature; LC = lesser curvature; AW = anterior wall side; PW = posterior wall side.
Table 2
Outcomes of the intrapyloric botulinum toxin injection

GOOSS = Gastric Outlet Obstruction Scoring System.
*GOOSS: 0) no oral intake; 1) only liquid diet; 2) soft solid diet; and 3) low residue or full diet; †Endoscopic food grade: 0) no residual food; 1) a small amount of residual food; 2) a moderate amount of residual food, but possible to observe the entire surface of the remnant stomach with body rolling; and 3) a large amount of residual food that hinders observation of the entire surface even with body rolling. Post-procedure endoscopy is performed at a median of 38 days after the botulinum toxin injection (range, 6–148 days); ‡Balloon pyloroplasty is performed before botulinum toxin injection, which does not improve the symptoms; §Mild anastomosis site stricture is observed.
Fig. 2
Upper gastrointestinal series and follow-up simple X-ray after botulinum toxin injection. (A) Pre-injection, (B) 2 days post-injection, (C) 4 days post-injection, and (D) 7 days post-injection. The nearly closed pylorus gradually opened (blue arrow), and the residual food in the stomach decreased after botulinum toxin injection. After 1 week, the pylorus widely opened, and the residual food emptied.
Four patients also received prokinetics after botulinum toxin injection (erythromycin for 1 week in 1 patient, metoclopramide and corydaline for 2 weeks in 2 patients, and corydaline for 2 weeks in 1 patient).
All patients underwent follow-up esophagogastroduodenoscopy at a median of 38 days after botulinum toxin injection (range, 6–148 days). The endoscopic remnant food grade of all 6 patients was 3 (a large amount) before the procedure, and 4 patients showed improvements in the endoscopic food grade from 0 (no residual food) to 2 (a moderate amount).
There were no immediate or delayed complications attributable to botulinum toxin injection. Two patients received additional botulinum toxin injections. One patient underwent one additional procedure due to a recurrence of symptoms, such as nausea and vomiting 5 months after the first botulinum toxin injection. The other patient showed little (grade 1) to no residual remnant food in 6 monthly endoscopic examinations after botulinum toxin injection; however, he strongly desired to receive repeated botulinum toxin injection due to indigestion recurrence at 6 months after each botulinum toxin injection. After a total of 5 botulinum toxin injections, he did not need further treatment.
The patients' median follow-up period was 27 months (range, 14.8−36.1 months). All patients were able to ingest normal regular diets at the last follow-up.
DISCUSSION
We have successfully managed postoperative delayed gastric emptying using botulinum toxin injection following PPG. The GOOSS score improved in all patients, and 5 of them were able to consume a soft solid diet within 10 days after the procedure. To our knowledge, this study is the first to report the use of botulinum toxin to alleviate delayed gastric emptying after PPG.
In refractory gastroparesis caused by diabetes and surgery and of unknown origin, the mean duration of botulinum toxin response was 5.1 months [7]. The duration of botulinum toxin effect (5−6 months) seems to be a sufficient time for the recovery of gastric emptying in most PPG patients. In an animal study, gastric stasis improved 1 month after resection of the pyloric branch of the canine vagus nerve, and the rate of gastric emptying after 1 month was similar to that of controls [5]. Humans may need a longer period for gastric emptying restoration compared to dogs [13]. Two patients required reinjection after 6 months from the first treatment, and both of their conditions improved again after botulinum toxin reinjection.
Recently, balloon dilation and/or retrievable stent insertion into the pylorus have been introduced for the treatment of patients with gastric stasis after PPG [14]. Overall, 73.3% of cases showed a good response to balloon dilation, and non-responders to balloon dilation were subsequently treated by a retrievable stent. However, balloon dilation or stent insertion frequently results in damages to the pyloric sphincter. Transmural tearing can develop with balloon dilation or stent insertion. Transmural tearing of the pylorus or pyloroplasty after PPG runs counter to the purpose of PPG, which is implemented to preserve the pylorus in contrast with subtotal gastrectomy. Moreover, patients require admission to the hospital for balloon dilation or stent insertion.
Botulinum toxin injection for the treatment of pyloric spasm has several advantages compared with balloon dilation and stenting. This procedure does not require fluoroscopic guidance. This procedure is easy and safe; thus, hospital admission for the procedure is not essential. Among a total of 11 sessions of botulinum toxin injections, 6 sessions were performed at outpatient clinics, and no complications developed after any session. A major advantage of botulinum toxin injection is that it does not damage the pyloric sphincter and permits time for natural recovery. Balloon dilation or stent insertion could be attempted if there is no improvement of symptoms with botulinum toxin injection.
Our study has several limitations. First, only 6 cases were enrolled. Therefore, it is difficult to evaluate the general efficacy of botulinum toxin injection in patients with delayed gastric emptying after PPG. In the future, a prospective study including a larger number of patients is needed to evaluate the efficacy of botulinum toxin. Second, the effect of botulinum toxin injection on gastric stasis was evaluated semi-quantitatively, based on the improvement of symptoms, diet grade, and endoscopic findings. A gastric emptying study as an objective evaluation method was not conducted. However, a gastric emptying study also lacks standardization to evaluate gastric emptying.
In summary, this study is the first to report the successful outcome of botulinum toxin injection in patients with delayed gastric emptying following PPG. We found that this technique could be an easier and more effective method than previous therapeutic trials. Further prospective studies are needed to determine the role of this treatment in patient management.
 XML Download
XML Download