

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Multiple early gastric cancer (MEGC) is easily overlooked during cancer surgery if not detected during preoperative endoscopic examination, and it can be the cause of remnant gastric cancer and positive resection margins [1]. According to Moertel et al. [2], multiple gastric cancers are defined as follows: 1) each lesion must be pathologically proven to be malignant, 2) all lesions must be distinctly separated by microscopically normal gastric walls, and 3) the possibility that one of the lesions represents a local extension or metastatic tumor must be completely eliminated. The incidence of MEGC has been reported to range between 4% and 11.7%. Compared to younger individuals, older individuals have a higher incidence of MEGC [3456]. Compared to solitary early gastric cancer (SEGC), MEGC more frequently accompanies intestinal metaplasia in the mucous membranes [6], although it is not related to lymph node metastasis [578] or prognosis [78].
Recently, the number of multiple primary malignancies detected in other organs has been increasing because of improved diagnostic technology, and increased lifespan and survival following operation [9]. The incidence of multiple primary cancers in other organs ranges between 2.04% and 3.4% [910]. The concept of field cancerization states that organ systems that have developed a neoplasm are likely to develop multiple and independent neoplasms, because all cells have been exposed to the same dose of carcinogens for the same duration of time [101112]. Field cancerization is thought as a possible mechanism of multiple gastric cancers and multiple primary malignancies in other organs; however, there are no reports on the correlation between the two. This study aimed to determine the clinicopathological features of MEGC and to investigate the correlation between MEGC and multiple primary malignancies.
MATERIALS AND METHODS
Of 3,107 patients with pathologically proven early gastric cancer (EGC) who underwent radical gastrectomy at Samsung Medical Center from January 2000 to December 2005, we retrospectively reviewed the medical records of 3,057 patients who had clinicopathological features of EGC and adequate medical records, and were available for postoperative follow-up. Follow-up was conducted through October 2010, and the mean follow-up period of all patients was 68.1±21.0 months. The mean follow-up duration for the SEGC and MEGC groups was 68.3±21.0 and 63.0±20.2 months, respectively. Follow-up observations were performed at 3 months, 6 months, and 1 year after surgery, after which the patients were followed up every year. Complete blood count, liver function tests, tumor markers, chest radiography, abdominal computed tomography (CT), and endoscopy were used as follow-up tests. Recurrences or multiple primary malignancies were evaluated by physical examination, chest radiography, ultrasonic inspection, colonoscopy, CT, and positron emission tomography (PET)-CT, and/or histological biopsy. Five years after surgery, patients were not routinely followed up in outpatient clinics, but they were recommended to undergo a mass screening test on a yearly basis. Our basic practice for gastrectomy entails radical resection of the primary tumor and D2 lymph node dissection under the Japanese Classification of Gastric Carcinoma. D1, D1+α, or D1+β was performed selectively in patients with a high operative risk, such as those with liver, lung, or heart disease, or in those who had undergone laparoscopic surgery [13]. According to Warren and Gates [14], multiple primary malignancies are defined by the following criteria: 1) each of the tumors must present a definite picture of malignancy, 2) each tumor must be distinct, and 3) the probability that even one of these lesions is a metastatic lesion must be excluded. According to Moertel [15], if a second tumor is discovered at the same time or within 6 months of the first tumor, it should be defined as a synchronous primary malignancy; if it is discovered after 6 months, it should be defined as a metachronous primary malignancy. The main lesion was defined as the largest lesion if the gastric wall invasion was the same.
IBM SPSS Statistics ver. 18.0 (IBM Corp., Armonk, NY, USA) was used for statistical analyses. Clinicopathological features were verified using the χ2 test, survival was analyzed using the Kaplan-Meier method, and significance testing was performed using the log-rank test. The Cox proportional hazards model was used for multivariate analysis.
RESULTS
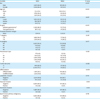
Among the 3,057 patients, there were 2,032 male patients (66.5%) and 1,025 female patients (33.5%), and their mean age was 55.6±11.4 years. MEGC was detected in 148 patients (4.8%), and it was more frequent in patients with the following characteristics: male sex (65.6% vs. 84.5%, P<0.001), old age (40.8% vs. 57.4%, P<0.001), total gastrectomy (11.2% vs. 25.0%, P<0.001), macroscopic type tumors (P=0.022), tumors less than 2 cm in size (70.1% vs. 61.5%, P=0.026), and differentiated-type tumors (58.1% vs. 68.9%, P=0.009). Fifty-three patients with SEGC (1.8%) and 5 patients with MEGC (3.4%) were found to have synchronous primary malignancies in other organs, but this difference was not statistically significant (Table 1). The percentages of accessory lesions located in the same anatomical region as the main lesions were as follows: 26.7% in the upper one-third, 64.7% in the middle one-third, and 54.9% in the lower one-third. Even with the macroscopic type, there was a tendency for agreement in type IIb (66.7%) and IIc (55.0%) lesions, and 95.1% of the lesions showed agreement when the main lesion was a differentiated-type tumor. The overall 5-year survival rates of SEGC and MEGC groups were 95.4% and 95.5%, respectively, and there was no statistically significant difference between the groups.
Table 1
Clinicopathological features in SEGC and MEGC
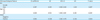
There was no difference in recurrence-free survival between the MEGC and SEGC groups, and the recurrent-free 5-year survival rates of SEGC and MEGC were 98.1% and 97.3%, respectively. MEGC was a risk factor for metachronous primary malignancies in other organs. During the postoperative follow-up, multiple primary malignancies were detected in 172 patients (5.6%), and the mean time interval of the diagnosis of the metachronous malignancies after gastrectomy was 54.0±3.4 months. Of these patients, 58 had synchronous multiple primary malignancies, and 114 had metachronous primary malignancies. Among the patients with SEGC, metachronous primary malignancy occurred in 102 patients (3.5%), and the median time to occurrence was 60.6±1.2 months. Multiple primary malignancies in the other organs occurred most frequently in the lung (n=33, 19.3%) and colorectum (n=29, 17.0%). Metachronous primary malignancies occurred in 12 patients with MEGC (10.5%), and the median time to occurrence was 51.0±2.8 months (Fig. 1). In univariate analysis for metachronous primary malignancies in the other organs, male sex (P=0.007), age greater than 60 years (P<0.001), and MEGC (P<0.001) were risk factors; there were no other differences in the clinicopathological findings (Table 2). In the multivariate analysis, male sex (P=0.027; hazard ratio [HR]=1.644), age greater than 60 years (P<0.001; HR=2.335), and MEGC (P=0.004; HR=2.444) were significant and independent risk factors for the development of metachronous primary malignancies after gastric cancer surgery (Table 3).
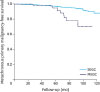
Table 2
Univariate analysis of the risk factors for metachronous primary malignancies after gastrectomy
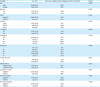
Table 3
Multivariate analysis of risk factors for development of multiple primary malignancies during follow-up of patients with gastric cancer
DISCUSSION
The pathogenesis of multiple gastric cancers remains unknown; however, synchronous tumors arising within a single organ may represent tumors of independent origin or, alternatively, may reflect lateral spread from a single source that results in multiple tumors with the same genetic alterations [16]. The clinicopathological features of multiple gastric cancers were more frequently observed in males, older patients, and patients with differentiated-type tumors. These results are consistent with those of previous studies [581718]. Therefore, we recommend that preoperative gastroscopy should be performed meticulously, especially in older men.
Similar to the findings of previous studies, we observed correlations among the location, macroscopic type, and microscopic type of accessory lesions [58]. Owing to similarities between the main lesion and accessory lesion, it is difficult to prove multicentricity in conventional pathologic studies on multiple gastric cancer [19]. Kang et al. [16] reported that the histologic type in multiple gastric cancer is related to loss of heterozygosity in APC and MCC, but not in p53. Additionally, they reported that loss of heterozygosity in APC and MCC does not occur in poorly differentiated adenocarcinomas. These findings indicate the existence of a multicentric origin, even if the main and accessory lesions have the same histologic or macroscopic features. Therefore, APC, MCC, or p53 mutations in the main and accessory lesion may not be the same, and this inconsistency supports a multicentric rather than a monoclonal origin for multiple gastric cancers. Sozzi et al. [11] suggested that specific genetic changes are discordant in multiple lung cancers, although the locations of the tumors or histologic diagnoses conformed to those of the main and accessory lesions. Inconsistencies such as these support the field cancerization theory, which states that multiple tumors occur from independent events resulting from the same carcinogenic exposure of multiple cells within the same organ or parenchymal field over the same time; multiple synchronous tumors of the upper aerodigestive tract are a well-known example [1011]. Age greater than 60 years and MEGC have been shown to be risk factors for metachronous primary malignancies. As long as the risk of cancer is constant, precancerous lesions are more likely to develop into clinical cancer in elderly individuals because of the longer duration of carcinogen exposure [12]. We believe that these findings add evidence to the field of cancerization hypothesis.
Multiple gastric cancers and solitary gastric cancer are known to have the same prognosis [78]. Kitamura et al. [7] attributed the difference in the survival rates between SEGC and MEGC to the high rate of complete cure for EGC, although missed accessory lesions may be fatal. Therefore, there are no significant differences in survival between the groups of patients with SEGC and MEGC, and the proportion of overlooked accessory lesions has decreased owing to the advancements in preoperative and intraoperative diagnostic examinations. Although MEGC was not a prognostic risk factor in our study, it was a risk factor for the development of metachronous primary malignancies. Dinis-Ribeiro et al. [20] reported that multiple primary malignancies in the other organs were detected in 3.4% of patients with gastric cancer and that 27% of them were synchronous, 73% were metachronous, and the most frequently associated tumors were colon cancer and breast cancer. Ryu et al. [21] reported that multiple primary malignancies were detected in 2.07% of patients with gastric cancer, and that 63% of them were synchronous and 37% were metachronous. In our study, multiple primary cancers were detected in 172 patients (5.6%), and metachronous primary malignancies were detected more often than synchronous primary malignancies. This could be attributed to the fact that the detection rate of metachronous primary malignancies increases with an extended follow-up period, and certain patients with EGC have a higher survival rate after gastric cancer surgery.
The pathogenesis of multiple primary malignancies has not yet been established. Watanabe et al. [22] reported that multiple malignancies occur mostly in the associated organs, and that the combination of multiple cancers that do not occur in organs such as the lungs and kidneys was the result of circulating carcinogens within the body. In our study, we found that lung cancer, liver cancer, and colorectal cancer were most commonly detected in patients with SEGC as the metachronous primary malignancy; in patients with MEGC, lung cancer and colorectal cancers, along with hematologic malignancies, were the most frequent primary malignancies. We believe that the metachronous primary malignancy was commonly detected in the non-adjacent organs (e.g., the lungs and the liver) in patients with MEGC, possibly owing to a circulating carcinogenic effect.
We believe that the metachronous primary malignancy was commonly detected in the patients with MEGC. Although MEGC was not a prognostic risk factor, it was a risk factor for the occurrence of metachronous primary malignancies after curative gastrectomy. Hence, when MEGC is diagnosed, careful observation of metachronous primary malignancies, especially lung cancer and colon cancer, is necessary during gastric cancer surveillance.
 XML Download
XML Download