

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Gastrointestinal stromal tumors (GISTs) are the most common primary mesenchymal neoplasms of the gastrointestinal tract.1 Although GISTs may occur throughout the gastrointestinal tract, approximately 60% of them originate in the stomach and 30% in the small intestine.2 GISTs usually appear as a discrete well-circumscribed but non-encapsulated mass with variable gross appearances, growing as intraluminal, extraluminal, or combination forms.3 Some GISTs present with circumscribed, mottled, or patchy calcifications similar to other tumors such as gastric cancer and hemangiomas with phleboliths.4 However, to our knowledge, GISTs showing a multilobular form with diffuse multifocal calcifications have not yet been reported. Here we report a case of gastric GIST presenting with a multilobular growth pattern with diffuse multifocal calcifications.
Case Report
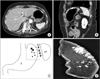
A 70-year-old female without a significant medical history visited Eulji University Hospital for a regular physical exam. She had denied any symptoms such as abdominal pain, melena, anorexia, or weight loss. The physical examination was unremarkable. Laboratory examination showed no abnormalities. An esophagogastroduodenoscopy showed a 2.0×2.0 cm protruding mass with normal overlying mucosa at the fundus in the stomach (Fig. 1A). Endoscopic ultrasound (EUS) revealed an ill-defined heterogenous hypoechoic lesion (3.0×1.5 cm) with multiple hyperechoic spots, arising from the muscularis propria layer (Fig. 1B). A computed tomography (CT) scan of the abdomen demonstrated a 4.5 cm multifocal calcified mass at the gastric body as well as at the gastric fundus (Fig. 2A, B). There were no enlarged perigastric or periesophageal lymph nodes. A preoperative evaluation led to the possible diagnosis of multifocal hemangiomas with phleboliths or a calcified GIST. A laparoscopic gastric wedge resection of the gastric fundus and high body was performed using linear stapler according to the maximal extent of multifocal calcifications that was shown on CT for tumor-free margin due to indistinct boundary of the tumor and discordant finding between endoscopy and CT (Fig. 2C). In addition, intraoperative mammography and frozen biopsy of the specimen was performed to confirm the complete removal of the excised specimen including the multifocal calcifications, and the specimen was compared to the preoperative CT finding (Fig. 2D). Calcification on the intraoperative specimen mammography was measured at 5.4×1.9 cm. The resected specimen revealed a well-circumscribed elongated mass measuring 5.2×2.0 cm, showing solid, whitish-yellow parenchyma (Fig. 3A). Histologically, the tumor that originated from the muscularis propria was extended longitudinally in multilobular form with diffuse calcifications (Fig. 3B). The tumor was composed of admixed spindle and epithelioid cells displaying finely vesicular chromatin and palely staining cytoplasm arranged in short intersecting fascicles and diffuse sheets (Fig. 3C). The mitotic rate was less than 5 mitoses per 50 high power fields and no prominent sign of nuclear atypia was seen. There was mild pleomorphism without necrosis. On immunohistochemical staining, the tumor cells were strongly positive for CD117 (Fig. 3D) and CD34, and negative for S-100 protein, alpha-smooth muscle actin, and desmin, and weakly positive for the DOG1 antibody. Since the size of this tumor was 5.2 cm (5~10 cm), the GIST was deemed an intermediate risk according to risk stratification guidelines.5 The postoperative recovery was uneventful and the patient was discharged eight days later.
Discussion
GISTs are currently thought to originate from the gastrointestinal pacemaker cells, the interstitial cells of Cajal, which are embedded in the musculature of the gastrointestinal tract. The majority of GISTs generally appear to be well-defined ovoid or round shaped masses, regardless of the size of the tumor. However, in our case, the GIST shows an ill-defined mass presented with a longitudinal and diffuse growth pattern along the muscular layer. Therefore, we can only presume the extent of the tumor through the calcification distribution due to the indistinct boundary of the tumor.
Endoscopic examination of a GIST generally shows a smooth subepithelial mass displacing the overlying mucosa and is useful to distinguish it from common gastrointestinal tract tumors, which usually originate in the mucosa. EUS is useful for estimation of size, origin, and invasion depth of the GIST. CT is considered to be the imaging modality of choice for the detection, staging, surgical planning, and follow-up of patients with GIST.6 However, in our case, the extent of the tumor could not be precisely localized through endoscopy, EUS, and CT due to the unusual longitudinal tumor growth pattern, with replacement of the muscularis propria. The only evidence for presuming the range of the tumor was the distribution of calcification shown on CT imaging.
Calcification is not rare in GISTs and is found in 3% of cases.4 It may also be present in other gastrointestinal tumors like mucinous gastric cancer and hemangiomas with phleboliths.7 Most cases of primary GIST with calcification that have been reported showed a solitary, punctuate, mottled, or patchy calcification pattern. 8 However, extensive dense calcification throughout the tumor 4 or diffuse multifocal distribution of calcification of GISTs is very rare in our case. Rege et al.9 reported that multifocal tumors with multinodular growth patterns typically arise in pediatric GISTs, not adult cases. No known relation currently exists between multifocal calcification and multilobular growth patterns.
The principles of surgical treatment for primary resectable GISTs are complete resection without causing tumor rupture, while acquiring negative margins.10 It is extremely important to avoid tumor rupture because it is associated with very poor outcomes, even in small GISTs with low mitotic counts.11 Generally, it is not difficult to decide the extent of resection because most cases show a well-circumscribed margin. However, in our case, we used the extent of the calcifications shown on CT as the only indicator for the smaller extent of resection, due to the unusual longitudinal growth pattern of GISTs.
In conclusion, we herein present the rare case of a gastric GIST showing a mutilobular form with diffuse multifocal calcifications, which was successfully treated by laparoscopic gastric wedge resection. In the case of an indistinct tumor boundary with calcification, intraoperative specimen mammography and frozen biopsy might be helpful to obtain a tumor-free resection margin. Additionally, in patients with diffuse multifocal calcifications of the stomach, the possibility of a GIST should be considered for the differential diagnosis.


 XML Download
XML Download