

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Tuberculosis (TB) is one of the leading infectious diseases, with a high morbidity and mortality worldwide; approximately 8.6 million new cases and 1.3 million deaths are reported annually.1 The incidence of TB in South Korea was 97 per 100,000 persons in 2010.1 The age-standardized incidence rate of gastric cancer is 59.3 persons and 23.5 persons per 100,000 male and female individuals, respectively.2 The co-existence of TB and cancer causes a diagnostic dilemma, as similarities in their presentations may lead to a delay in the appropriate therapy.3 In the current patient, a diagnosis of gastric cancer was established. However, the finding of peritoneal nodules, lymphadenopathy, ascites, and left pleural effusion with a suspicion of TB caused a treatment dilemma due to difficulties in making a differential diagnosis between advanced cancer with peritoneal carcinomatosis (PC) and TB pleurisy and peritonitis.
Case Report
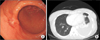
The patient was a 39-year-old married woman who presented to her local hospital with a history of abdominal pain and heartburn. There was no history of fever or contact with TB patients. She complained of a cough and grade 2 dyspnea with no hemoptysis. Physical examination revealed dullness with decreased air entry in the left lower chest and a soft abdomen with no rigidity or palpable masses. She had a Bacillus Calmette-Guérin vaccination scar. An upper gastrointestinal (GI) endoscopy revealed a 2-cm ulcerative early gastric cancer in the antrum, with a biopsy result of signet ring cell carcinoma (Fig. 1). Chest radiography and chest computed tomography (CT) revealed a left pleural effusion with pleural nodularity and lymphadenopathy (Fig. 1).
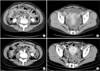
An abdominal CT scan revealed diffuse peritoneal thickening, lymphadenopathy, a small amount of ascites, and nodular omental infiltration, suggesting a diagnosis of PC over that of tuberculous peritonitis (TBP) (Fig. 2). Positron-emission tomography revealed left pleural and peritoneal hyper-metabolic lesions, most likely representing metastasis. Thoracentesis revelaed a dominant lymphocytic exudate, with an adenosine deaminase (ADA) level of 145.5 units/L, which was consistent with TB pleurisy. The results of an acid-fast bacilli smear and tuberculin test were negative.
The patient subsequently presented to our hospital for a second opinion. Repeat thoracentesis with biopsy was performed; the cytological analysis showed lymphocytic exudate, and the histology consisted of chronic inflammation with necrosis, suggesting TB pleurisy. Paracentesis was not possible due to the small amount of ascites. The levels of the serum tumor markers cancer antigen (CA) 125 and CA 72-4 were 107 units/ml and 3 units/ml, respectively. Her carcinoembryonic antigen (CEA) level was 1.7 ng/ml.
These findings, in addition to the gastroscopic diagnosis of early gastric cancer, raised the possibility of TBP rather than PC. We therefore decided to start anti-TB medication for 2 weeks initially, in order to avoid the active phase and infectivity of TB; we then planned to compare the amount of pleural effusion and abdominal findings such as ascites, lymphadenopathy, and omental infiltration after this period. A follow-up CT scan revealed increased pleural effusion and little improvement in the abdominal findings (Fig. 2). We next planned a laparoscopic exploration with a frozen biopsy to confirm the diagnosis. The intraoperative macroscopic view was suggestive of TBP, and the frozen biopsy of several random peritoneal nodules showed chronic granulomatous inflammation (Fig. 3). Hence, a laparoscopic distal gastrectomy with lymph node dissection was performed. The final pathological diagnosis was stage Ia early gastric cancer according to the American Joint Committee on Cancer staging system 7th edition (sub-mucosal invasion and no metastasis in 26 harvested lymph nodes), and it was associated with chronic granulomatous inflammation and necrosis in the perigastric lymph nodes. The patient was discharged on postoperative day 7 on anti-TB medication and had an uneventful postoperative period. She visited our outpatient clinic 2 months later with no complaints.
Discussion
Patients with malignant diseases are at an increased risk of TB. However, the association of TB with cancer could be coincidental or result from a secondary infection due to immunosuppression from chemo or radiotherapy. Old age, male sex, previous anti-TB treatment, and gastrectomy are significant risk factors for TB.4 An increased risk of TB incidence after chemotherapy has been observed in patients with a history of TB.4 This is important, as TB involvement of the genitourinary or GI tract, peritoneum, lymph nodes or viscera constitutes up to 12% of extra-pulmonary TB cases, and its nonspecific symptoms and signs may mimic GI or ovarian cancers.5 TBP is divided into three overlapping types: wet type (the most common, ~90% of cases), dry type, and fibrotic-fixed type.
A diagnosis of adenocarcinoma with signet ring cells in a young woman is a risk factor for a poor prognosis.6 In our young female patient, signet ring cell gastric cancer with peritoneal thickening and nodules, lymphadenopathy, and ascites caused a diagnostic dilemma between PC and TBP, two diseases with completely different treatment pathways and prognoses. There are no pathognomonic clinical features or imaging findings that enable a definite diagnosis of TBP. Therefore, TB involvement of the peritoneum can be easily confused with PC. Clinical findings such as a duration of symptoms and fever of less than 1 month are helpful for differentiating TBP from PC.7 Some authors suggest that polymerase chain reaction on the ascitic fluid obtained by ultrasound-guided fine needle aspiration is a relbiale method for TB diagnosis and should at least be attempted before surgical intervention.8 However, this was difficult in our case owing to minimal ascites.
In addition to clinical and radiologic findings, an ascitic fluid ADA measurement is also helpful in the differential diagnosis of TBP and PC.7 The role of tumor markers is not clear owing to a lack of specificity and sensitivity. In a previous study, theu tahors attempted to differentiate TBP from PC in 75 patients based on many parameters including tumor markers. They concluded that, in the absence of other systematic diseases, the presence of a fever, an elevated serum CA 125 level, and normal serum CA 19-9 and CEA levels associated with predominantly benign ascites with lymphocytes may establish the diagnosis of TBP.7 In our patient, anti-TB medication was started 2 weeks before surgery for diagnostic purposes, based on the response to treatment (an improvement of the peritoneal signs and the pleural effusion would indicate TB over PC), and to render the infective phase non-infective in the case of TB. We believe that laparoscopic exploration and histology on frozen sections may be the best approach for establishing the diagnosis and starting the appropriate treatment in such patients in the future. Laparoscopy is the diagnostic tool of choice in patients with suspected TBP.9 Co-existence of both TB and gastric cancer does not constitute a contraindication for anti-TB and anti-cancer chemotherapy, although chemotherapy was not indicated in our present case.10
In conclusion, the symptoms and signs of peritoneal TB are non-specific, and clinicians should adopt a high level of suspicion for peritoneal TB in patients who are febrile with the symptoms and signs of pulmonary TB, who have a history of TB, or who live in an area with a high incidence of TB. Tissue biopsy or laparoscopic exploration is preferred for diagnosing such cases. Early diagnosis is critical for the management and prognosis of these patients, and there seems to be no contraindication for combined treatments.

 XML Download
XML Download