

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Gastrointestinal stromal tumor (GIST) is one of the most common sarcomatous tumors detected in gastrointestinal tract.1 The incidence of GIST is 7 to 10 cases per million people in -Eu rope and the USA.23 However, in Korea, the incidence is higher than that in Europe or the USA, a 16 to 22 cases per million people.4
GISTs are derived from interstitial cells of Cajal, and they have three histological types, spindled, epithelioid, and mixedtype cells.5 Identifying the expression of CD117, also known as kit, by immunohistochemical (IHC) staining is necessary to diagnose GISTs. CD117 expression can be found in over 95% of GISTs.6 However, CD117 expression is not found in the 5% of c-kit-negative GISTs. Although, in those cases, additional staniing with Discovered on GIST-1 (DOG1, also known as ANO1) can be helpful to confirm a GIST,7 the diagnosis and treatment of c-kit negative GISTs remain obscure.
Here, we have encountered a c-kit-negative GIST case, and we are going to report on the diagnosis and treatment of that tumor.
Case Report
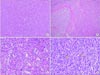
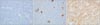
A 73-year-old man presented with abdominal distention and maldigestion for 1 month. The patient had a medical history of diabetes and hypertension. An intraabdominal mass was palpated in the epigastric area, and the patient did not complain of pain and tenderness. Laboratory findings showed no abnormalities, except an elevated fasting glucose level. Contrast-enhanced computed tomography (CT) revealed an 18-cm exophytic mass from the anterior wall of the lower body of the stomach without regional enlarged lymph nodes (Fig. 1). The patient underwent mass removal by gastric wedge resection. The resected specimen was an 18.0×15.0 cm, irregularly shaped, multi-lobulated, yellow, soft, and fleshy mass with a 3.5×2.5 cm wedge-resected portion of the stomach (Fig. 2). The tumor directly invaded the adjacent adipose tissue, grossly. Microscopically, a routine H&E-stained section showed a hypercellular tumor lesion with diffuse sheet-like growth patterns under low-power magnification (Fig. 3A). Some portions of the tumor showed hyalinized stroma with slit-like vessels and sinusoidal capillaries around the tumor cell nests (Fig. 3B). At higher magnification, tumor cells were epithelioid and had prominent cytoplasmic vacuoles and uniform nuclei with moderate nuclear pleomorphisms (Fig. 3C). Mitotic figures were counted in the most active area ('hot spots'), and 37 mitoses per 50 high-power fields (HPFs) were observed (Fig. 3D). By IHC staining, tumor cells were negative for CD117 (Fig. 4A) and CD34 (Fig. 4B). However, DOG1 was observed in the membrane and cytoplasm of the tumor cells (Fig. 4C). There was no involvement of the resected margins. Consequently, this tumor was diagnosed as a c-kit negative GIST with a high risk of malignant behavior. Post-operative recovery was uneventful, and the patient was discharged on post-operative day 7.
Discussion
The stomach is the most common organ (50% to 60%) in which GISTs are found. The other organs are the small intestine (30% to 35%), colon (5%), and esophagus (<1%). Less than 5% of GISTs are found in the omentum, mesentery, and retroperitoneum, and those tumors are called extra-GISTs (E-GISTs). EGISTs occur in relatively high proportions in Korea (10%).8
In fact, the identification KIT or PDGFRA mutation by gene analysis is needed to make a confirmatory diagnosis. In general, the identification of CD117 expression by IHC staining is enough to diagnosis GISTs, clinically. Moreover, CD117 or CD3 4 expression is found in more than 90% of GISTs.8 However, they are not expressed in some GISTs. In CD117- or CD34-negative cases, DOG1 expression could be identified if the patients are clinically suspected of having GISTs. DOG1 expression is detected in many c-kit-negative GISTs,8 and one previous study reported that more than 90% of c-kit-negative GISTs were positive for DOG1.9 Several studies have reported that DOG1 is more sensitive than CD117 and more helpful, especially in ckit- negative GISTs.101112 Thus, for patients who are clinically su-s pected of having c-kit negative GISTs, DOG1 expression should be checked.
C-kit-positive GISTs are treated with surgery and/or imatinib. Imatinib is prescribed for patients with GISTs based on their risk of recurrence or metastasis, which is estimated using tumor size and the number of mitoses. In the stomach, for low-risk GISTs, which are less than 2 cm and have less than 5 mitoses per 50 HPF, a complete (R0) resection without rupturing is recommended.13 Lymph node dissection is usually not recommended. For high-risk GISTs, which are larger than 2 cm or have more than 5 mitoses per 50 HPF, a complete resection, if possible, is recommended following adjuvant imatinib. For unresectable GISTs, neoadjuvant or palliative imatinib and/or surgery is recommended.14 For c-kit-positive GISTs, 400 mg daily imatinib can be used for neoadjuvant, adjuvant, and palliative treatment.1516
Despite these treatment modalities, the 5-year survival rate o f c-kit-positive GISTs is known roughly to be 48% to 65%, and the tumors usually recur. The prognosis of GISTs depends on tumor size, the number of mitoses, chemotherapy, and complete resection.17 On the other hand, the prognoses and predictive fa-c tors for prognosis of c-kit-negative GISTs remain unclear.
However, complete resection and adjuvant imatinib, if possible, should be considered for c-kit-negative GISTs also because of the possibility of KIT or PDGFRA mutation, as in c-kitpositive GISTs.18 Imatinib is a competitive inhibitor of tyrosine kinases, such as KIT and PDGFRA,19 and several studies have shown that the c-kit-negative GISTs still have mutated KIT or PDGFRA despite the absence of IHC expression.18 Therefore, surgery and imatinib should be used as a therapeutic strategy for c-kit-negative GISTs. In addition, some studies reported the effectiveness of imatinib.7 However, c-kit-negative GISTs commonly have PDGFRA D842 mutations, and in such cases, imatinib resistance develops.9 Thus, clinicians should consider this mutation when considering imatinib treatment for c-kitnegative GISTs.
We reported on our patient with a c-kit-negative GIST. The tumor, which was located in the stomach, was completely resected in spite of its large size. The histological diagnosis was confirmed with DOG1 IHC staining. According to the indications for imatinib, the patient should have been treated with adjuvant imatinib, based on the risks of the tumor. However, the patient refused further evaluation and imatinib treatment for rpivate reasons. Recurrence has not yet developed, as of 9 months after surgery. If the patient is treated with adjuvant imatinib, a lower recurrence rate can be expected.


 XML Download
XML Download