

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
It is well known that the most common sites of gastric carcinoma recurrence are the liver, lungs, lymph nodes, and peritoneum.1 Although metastasis to the posterior mediastinal lymph nodes is occasionally encountered after gastrectomy, recurrence in the anterior mediastinum is extremely rare. We report a very rare case of a single thymic metastasis from gastric cancer occurring 5 years after a distal gastrectomy with lymph node dissection.
Case Report
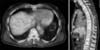
An asymptomatic 67-year-old man had a history of gastric adenocarcinoma (Fig. 1), for which he had undergone a distal partial gastrectomy 5 years previously. Histological examination of the resected specimen had revealed moderately differentiated adenocarcinoma invading the muscularis propria with 5 regional lymph node metastases at stations 1 (3/7), 3 (1/1), and 7 (1/1). The disease was stage IIB as defined by the Japanese Gastric Cancer Association.2 The patient received postoperative adjuvant chemotherapy with the oral fluoropyrimidine S-1 (100 mg/body). However, he could only take 1 course of chemotherapy because of severe diarrhea.
Four years and 8 months after the initial operation, a computed tomography scan from the chest to the pelvis demonstrated a tumor in the anterior mediastinum (Fig. 2). With 18F-fluorodeoxyglucose positron emission tomography computed tomography, a focal hypermetabolic lesion with a maximum standardized uptake value of 3.6 was identified in this lesion (Fig. 3). The patient underwent an anterior mediastinal tumor resection by video-assisted thoracic surgery (Fig. 4); the preoperative diagnosis was thymoma, thymic carcinoma, or malignant lymphoma in the thymus. Histopathology of the tumor revealed adenocarcinoma cells that were similar to those of the gastric cancer resected 5 years previously. Furthermore, immunochemistry indicated that tumor cells were positive for cytokeratin 20 and CDX-2 (C and D) and negative for cytokeratin 7.
Thymic metastasis was considered likely based on the location of the tumor (Fig. 5). The patient is currently taking the oral fluoropyrimidine S-1 (100 mg/body) as adjuvant chemotherapy to prevent recurrence.
Discussion
In this report, we describe a solitary thymic metastasis from a previously resected gastric cancer, which is an extremely rare occurrence. The thymus is an essential organ that controls cellular immune function; therefore, it has been considered almost impossible for a tumor to metastasize to it. However, detailed study of the thymic structure has revealed that it is not absolutely safe from tumor metastasis.3 As described by Clark,4 the parenchyma of the thymus is associated with a blood-thymus barrier that prevents it from making direct contact with antigens or cancerous cells, thereby seemingly excluding the occurrence of cancer metastasis. However, the septum of the thymus comprises interlobular connective tissue with blood vessels, lymph ducts, and nerves that theoretically enable contact with other parts of the body through the blood and lymphatic systems.
There are relatively few reports3,5,6,7 of thymic metastases, but gastric, breast, laryngeal, and lung carcinoma metastasis to the thymus has been reported at autopsy.8 In an autopsy series by Middleton,8 7 cases of thymic metastasis occurred in 102 carcinoma cases, which is an incidence of approximately 7%. There was only 1 case of gastric cancer among these 7 cases. To our knowledge, no antemortem cases of thymic metastasis from gastric cancer have been previously reported.
In our case, thymic structures could not be recognized around the tumor. This is reasonable because the thymus degenerates after adolescence and is replaced by fatty tissue. Therefore, our conclusion that the tumor originated in the thymus is based on the metastatic tumor's location.
It is important to detect metastatic tumors as soon as possible because some patients can be successfully palliated with appropriate treatment and may even achieve prolonged survival. The recognition that gastric cancer can metastasize to unusual sites, such as the thymus, can facilitate an accurate, prompt diagnosis and appropriate treatment.




 XML Download
XML Download