

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
As the population has aged, life expectancy has increased to 77.9 years for males and 84.6 years for females in Korea.1 Although the overall incidence of gastric cancer has decreased, the incidence in the elderly is increasing. The morbidity and mortality rates after gastric cancer surgery are reportedly 43% to 46% and 10% to 13%, respectively, in Western countries.2,3 In contrast, large-scale studies in Korea have reported morbidity and mortality rates of 12.5% to 17.4% and 0.3% to 0.6%, respectively, after gastric cancer surgery.4,5
The only effective and proven method for management of patients with clinically resectable gastric cancer is curative resection of the primary tumor and proper lymph node dissection. However, this is not an easy process for elderly patients, as they commonly have various comorbidities such as hypertension, diabetes mellitus, cardiovascular disease, pulmonary disease, and cerebrovascular disease, all of which extend the postsurgery recovery period. Furthermore, studies have reported that comorbidities are significantly related to morbidity after gastric cancer surgery.6,7 Surgeons cannot avoid all postoperative complications, and these issues must be effectively managed when they occur.
The rate of postoperative complications has decreased over time due to improvements in anesthesiology, surgical instruments, operating techniques, perioperative nutritional support, and careful preoperative evaluations. The current study evaluated clinicopathological characteristics and operation risk factors related to older age and management of postoperative complications following gastric cancer surgery in elderly patients.
Materials and Methods
A total of 420 patients with gastric adenocarcinoma underwent gastric resection in the Department of Surgery at our institution between March 2010 and January 2013. Of the 420 patients, 411 patients met the following study criteria: curative resection with D1+ or ≥D2 lymph node dissection, no history of other organ malignancies, and >15 retrieved lymph nodes.
Patients with stage IV gastric cancer were excluded. Two surgeons verified the levels of the dissected lymph nodes, and pathologists examined all retrieved lymph nodes for metastasis. Subtotal or total gastrectomies were performed, and the negativity of resection margins for tumor invasion was confirmed. Laparoscopic or robotic surgery was performed for patients with gastric cancer in early clinical stages. Combined resection was considered for patients with visualized local invasion into the adjacent organs including the spleen, distal pancreas, transverse colon, or gallbladder. The extent of lymph node dissection was defined according to Japanese Research Society for Gastric Carcinoma recommendations. Cancers were staged according to the tumor-node-metastasis classification system from the Union for International Cancer Control (UICC).8 Potentially curative resection was defined as R0 resection according to the UICC residual tumor classification system. The elderly group in this study included patients who were ≥70 years of age. Postoperative morbidities were assessed by physical examinations, routine laboratory tests, and radiological examinations during hospitalization. Hospital mortality was defined as postoperative death within 30 days or death during hospitalization. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). Patients were categorized as either non-overweight (BMI<25 kg/m2) or overweight (BMI≥25 kg/m2).
We compared clinicopathological variables and perioperative factors (operation time, time to first flatus, time to initiation of a soft diet, number of metastatic and retrieved lymph nodes, and postoperative hospital stay length), postoperative morbidities, and the hospital mortality rate for each age group.
1. Statistical analysis
Statistical analyses were performed using Statistical Package for the Social Sciences software, version 15.0 for Windows (SPSS Inc., Chicago, IL, USA). Clinicopathological variables were analyzed using chi-squared tests for discrete variables or Student's t-tests for continuous variables. The risk factors that influenced postoperative complications were determined using logistic regression analysis. P-values <0.05 were considered statistically significant.
Results
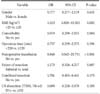
The clinicopathological characteristics of the 411 patients are summarized in Table 1. The mean patient age was 61.3 years (range, 23~90 years). There were 119 patients (29.0%) in the elderly group. The 2 groups were evenly distributed and did not differ in terms of gender, BMI, tumor size, invasion depth, lymph node involvement, extent of lymph node dissection, or extent of gastrectomy. However, the elderly group had a higher prevalence of comorbidities than the non-elderly group. The most common comorbidity was hypertension (125 patients, 30.4%), followed by pulmonary diseases (20 patients, 4.9%), diabetes mellitus (19 patients, 4.6%), heart diseases (13 patients, 3.2%), and liver diseases (12 patients, 2.9%). The elderly group more frequently had tumors located in the upper third of the stomach (24.4%) compared to the non-elderly group (13.4%). Intestinal-type tumors were also more prevalent in the elderly group (63.0%) compared to the non-elderly group (54.5%). In the elderly group, combined resection and conventional operations were performed more commonly, and intraoperative and postoperative transfusions were required more frequently. Although the mean operation time was significantly shorter in the elderly group (216.3 vs. 239.6 minutes), the time to first flatus (3.5 vs. 3.2 days) and the time to initiation of a soft diet (7.2 vs. 6.7 days) were longer in the elderly group, as was the length of postoperative hospital stay. There were no significant differences between the age groups in the number of lymph nodes that were metastatic (3.6 vs. 4.0 nodes) or retrieved (44.3 vs. 46.6 nodes) (Table 2).
Postoperative complications occurred in 53 patients (12.8%) and were significantly more common in the elderly group. Hospital mortality (5/411 patients, 1.2%) only occurred in the elderly group. The 5 mortalities were attributable to sepsis due to bile peritonitis, sepsis due to intra-abdominal fluid collection with abscess, sepsis due to anastomotic leakage, myocardial infarction, and pneumonia with cerebral infarction, respectively. Non-surgical complications such as atelectasis, pneumonia, pleural effusion, or myocardial and cerebral infarction were predominantly found in the elderly group (P<0.001). Other surgical complications such as wound infection, fluid collection, intraluminal bleeding, intestinal obstruction, ileus, anastomosis leakage, duodenal stump leakage, pancreatic fistula, and hepatic complication were evenly distributed between the 2 groups (P=0.463). Four patients in the non-elderly group had stenosis of the anastomotic area, while 1 patient in the elderly group had a remnant stomach perforation (Table 3). The numbers of grade I, II, IIIa, IIIb, and V complications according to the Clavien-Dindo classification system were 11 (2.7%), 31 (7.5%), 4 (1.0%), 2 (0.5%), and 5 (1.2%), respectively.
The complication rates were similar in patients with differences in gender, BMI, comorbidities, operation time, preoperative and intraoperative transfusion, extent of resection, combined resection, extent of lymph node dissection, tumor size, invasion depth, lymph node metastasis, and surgeon. Logistic regression analysis showed that postoperative morbidity was significantly associated with old age and postoperative transfusion (Table 4). High BMI and postoperative transfusion were important factors for postoperative complications in the elderly group (Table 5).
Discussion
In the past, the resection rate of elderly patients with gastric cancer was very low in Europe (25%~50%) compared to Japan (56%~83%).9,10 More recently, resection rates have increased due to the widespread availability of endoscopy technology,11 which leads to earlier gastric cancer diagnosis combined with improved surgical skills, anesthesia, and postoperative intensive care.
In most countries, a person >65 years old with decreased socioeconomic function, functional loss of major organs, or decreased ability to recover from stress such as trauma is defined as 'elderly.' However, there are no clear criteria for defining this group. Elders are sometimes divided into subgroups: young-old (65~74 years), old-old (75~84 years), and oldest-old (≥85 years).12 Some papers have reported that >30% of patients with gastric cancer are >70 years old.13,14 Furthermore, a study found that pulmonary dysfunction was significantly associated with patients ≥70 years old compared to patients <70 years old.15 Therefore, we defined elderly gastric cancer patients as those >70 years old, because they accounted for approximately 30% of gastric cancer patients, which allowed us to obtain a sufficient sample size to achieve statistical significance. Moreover, raising the age criteria in the elderly group did not yield significant results due to the small sample size.
Most surgeons are reluctant to operate on elderly patients due to high morbidity and mortality rates. Improvements in surgical techniques and anesthesia have made gastrectomies safer for elderly patients with gastric cancer, but postoperative morbidity and mortality rates remain high.15,16 In this study, we also found that the postoperative morbidity rate was higher in elderly compared to non-elderly patients (22.7% vs. 8.9%). Moreover, the recovery period of elderly gastric cancer patients who underwent gastrectomies was longer in terms of bowel movement, start of soft diet, and hospital stay. However, some studies have shown no differences in postoperative outcomes between elderly and young patients.17,18,19 Furthermore, minimally invasive surgery has been widely adopted for elderly patients with gastric cancer, and it has a shorter recovery period than conventional surgery as well as similar postoperative morbidity rates as those experienced by young gastric cancer patients.20 In this study, most elderly patients had more than 1 comorbidity including hypertension (30.4%), pulmonary disease (4.9%), diabetes mellitus (4.6%), and coronary and heart disease (3.2%). Moreover, when our department first started performing laparoscopic gastrectomies for elderly patients, we had to exercise caution because the lack of an experienced laparoscopist and assistant could lead to prolonged operation times. Prolonged carbon dioxide insufflation into the intra-abdominal cavity can damage the cardiopulmonary physiology in elderly patients with comorbidities.21
Some reports have indicated that total gastrectomies and extended lymph node dissections were associated with high surgical morbidity and mortality rates in gastric cancer patients.22,23 Limited lymph node dissection is frequently performed in elderly patients but does not seem to affect their disease-specific survival rate.24 Careful preoperative assessments of organ function and limited lymph node dissection may explain why there are fewer postoperative complications in elderly patients.24 However, we performed extended lymph node dissections in patients with advanced disease for curative surgery, regardless of age, because D2 dissection is the standard at our institute and our 2 surgeons are very experienced with this procedure. The mean number of retrieved lymph nodes in the elderly group was >40, which was not significantly different from the non-elderly group. Moreover, our study showed acceptable complication rates with regard to the extent of resection and lymph node dissection. The connective tissue and lymph nodes of elderly patients are susceptible to easy bleeding during surgery. Therefore, elderly patients are likely to lose a significant amount blood and require transfusions. Transfusions are associated with risks including transfusion-related acute lung injury, multiple organ failure, graft-versus-host disease, and infectious disease transmission.25 Several reports have shown that perioperative transfusions increase postoperative complications,26,27 whereas other studies have shown the opposite to be true.28
In the present study, although there was no significant difference in major surgical complications between the 2 groups, the frequency of intraoperative and postoperative transfusions was significantly higher in the elderly group, as was the incidence of non-surgical complications including atelectasis, pneumonia, and pleural effusion. We also found that old age, comorbidities, and advanced gastric cancer were risk factors for perioperative transfusion (data not shown). The prevalence of obesity in the elderly is growing gradually in our aging society. However, the relationship between obesity and surgical outcomes remains debatable. Some studies in Western countries have reported that obesity is only a simple predictor of wound infection and not a risk factor for major postoperative complications.29 However, evidence in Asian populations suggests that high BMI correlates with increased postoperative complications.30 We found that higher BMI was not a risk factor for postoperative complications. However, subgroup analysis of the elderly group revealed that higher BMI was a risk factor for postoperative complications.
Based on our results, it is difficult to conclude that abnormal pulmonary function or surgical complications are the causes of pulmonary complications in elderly patents. However, postoperative pulmonary problems are more common in elderly patients, as they tend to have chronic obstructive pulmonary disease, have smoked long-term, and have a poor general health status. Therefore, it is necessary to minimize postoperative pulmonary complications by optimizing perioperative lung function using methods such as deep breathing exercises, incentive spirometry, and epidural anesthesia.31
Limitations of this study include the retrospective nature of the study and an inaccurate amount of intraoperative blood loss. Despite these drawbacks, this study demonstrated that perioperative transfusion was an important risk factor for surgical complications in elderly patients with gastric cancer. Another limitation is that we were not able to show long-term surgical outcomes of elderly patients with gastric cancer because our institution is relatively new. Long-term follow-up data will be collected for future analysis.
In conclusion, pulmonary complications were frequent problems in elderly patients after gastric cancer surgery. Higher BMI and perioperative transfusion, particularly postoperative transfusion, were significant risk factors for postoperative complications in elderly patients with gastric cancer.




 XML Download
XML Download