

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Accurate pre-operative diagnosis is a prerequisite for optimal treatment planning in gastric cancer. Furthermore, in advanced gastric cancer (AGC), it is important that adjacent organ involvement be detected pre-operatively to enable patients to be properly informed and to avoid unnecessary resection. Extended local resection in AGC has been reported to increase survival, but also substantially increases morbidity, and thus, adequate information on adjacent organ involvement can helpfully decrease morbidity.(1,2)
The sensitivities of multidetector computed tomography (CT) and endoscopic ultrasound (EUS) for adjacent organ invasion have been reported to be slightly in excess of 60%.(3-5) On the other hand, the sensitivity of staging laparoscopy for metastatic lesions, in terms of peritoneal seeding or liver metastasis, is 91.7%, but its sensitivity for adjacent organ involvement is only 40%.(6) Thus, another useful tool or marker for detecting adjacent organ involvement is required.
Fibrinogen is a 340-kDa protein, that is converted to fibrin by the proteolytic action of thrombin, which is primarily produced by the liver.(7) In addition to its well-known roles in blood coagulation, recent studies have shown that fibrinogen plays important roles in a variety of processes, which include cell-to-cell interactions, inflammation, and cancer progression.(7-9) Elevated fibrinogen can enhance augment lymphatic and hematogeneous metastasis of advanced gastric cancer, which is major determinant of the prognosis in T2 gastric cancer.(10) In a previous study, we found that pre-operative plasma fibrinogen level is a useful marker of extent of tumor progression in gastric cancer.(11) However, few studies have evaluated the relationship between pre-operative plasma fibrinogen levels and tumor extent in gastric cancer.
Accordingly, the present study was undertaken to assess the association between pre-operative plasma fibrinogen levels and adjacent organ involvement in advanced gastric cancer.
Materials and Methods
In the present study, we retrospectively analyzed a prospective gastric cancer database. From April 2001 to December 2005 (inclusive), 945 patients considered clinical AGC (more than clinical T2) underwent gastric resection at the Center for Gastric Cancer, National Cancer Center, Korea. Ten double primary cancers and 12 with other cancer history were excluded to avoid bias in the present study. As a result, 923 patients were included in this study. The pre-operative diagnostic tools used were esophagogastroduodenoscopy (EGD) with biopsy, abdominal and pelvic CT, chest radiography, and a basic blood testing including fibrinogen level as institutional guidelines.(12,13) Pre-operative fibrinogen levels were measured before surgery using 5 ml whole blood samples drawn from an antecubital vein using a tourniquet, a 20-gauze Vacutainer needle, and a 3.8% sodium citrate Vacutainer collection tube (Becton Dickson, Rutherford, NJ, USA). Fibrinogen levels were quantified by immunoassay (Coagrex 800®, Shimadzu Corporation, Kobe, Japan).
The present study was performed in accordance with the guidelines issued by our institutional review board, which approved the study protocol and waived the requirement for informed consent. All patients provided informed consent for surgery.
EGD with biopsy, abdominal and pelvic CT, chest radiography, and basic blood testing. An upper gastrointestinal study and endoscopic ultrasound were performed when needed. Only patients with T2 or more disease according to pre-operative findings were enrolled in this study. Pre-operative T staging of gastric cancer by CT was classified as follows: T1, non-transmural enhancement with focal wall thickening or marked enhancement only without wall thickening; T2, transmural enhancement with focal wall thickening, smooth outer border of the thickened gastric wall; T3, nodular or irregular outer border of the thickened gastric wall or blurred fat plane around the lesion or perigastric fat infiltration; and T4, gross infiltration of adjacent organs.(14,15)
The surgical procedures and reconstruction methods were standardized, as follows. Distal subtotal gastrectomy was performed if a tumor-free margin of 5 cm was present in cases with advanced gastric carcinoma or of 2 cm in cases with early gastric carcinoma. Extent of lymph node dissection was determined using the recommendations of the Japanese Research Society for Gastric Carcinoma.(16) After laparotomy, surgeons examined intra-abdominal cavities and inspected peritoneum, diaphragms, liver capsules, and pelvic cavities. When a main lesion was suspected to be over T3, peritoneal washing cytology was performed. All patients enrolled in the present study underwent gastrectomy with D2 lymph node dissection. More than 15 lymph nodes were retrieved from all patients. Tumors were staged, in accordance with the 6th Union International Centre Cancer tumor node metastasis classification,(17) and added Lauren classification.(18)
1. Statistical analysis
Various clinicopathologic and therapeutic factors, including fibrinogen level, were analyzed using the Chi-square test and the student's t-test. Spearman's rank correlation coefficients were used to examine associations between pairs of variables. Independent variables were entered into a logistic regression model to examine the nature of the relation between fibrinogen level and adjacent organ involvement. Survival was estimated using the Kaplan-Meier method with the log rank test. The statistical analysis was carried out using SAS version 9 (SAS Institute Inc., Cary, NC, USA). All P-values were two sided, and statistical significance was accepted for P-values of less than 0.05.
Results
1. Patient characteristics
The characteristics of the study population are listed in Table 1. The median age of the 923 patients was 60 years (range; 49~67 years), and there were 624 (67.6%) males and 299 (32.4%) females. Median tumor size was 5.5 cm (range 4.0~8.0 cm), and 805 (87.2%) patients were found to have AGC by pathologic examination.
2. Fibrinogen levels and correlations with clinicopathologic factors
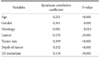
The median fibrinogen level was 327.0 mg/dl (Interquartile range, IQR 273.0~407.0 mg/dl). Two hundred and forty nine (27.3%) patients had an elevated fibrinogen level (>400 mg/dl). Elevated fibrinogen level was found to be positively correlated with the following clinicopathologic parameters; age, tumor size, depth tumor, and lymph node metastasis (P<0.001) (Table 2).
3. Associations between adjacent organ involvement and clinicopathologic factors and fibrinogen levels
Table 3 shows univariate analysis results for relations between clinicopathologic factors and adjacent organ involvement, which was present in 50 (5.4%) patients. The following were found to be associated with adjacent organ involvement; lymphatic invasion (P<0.001), tumor size (P<0.001), clinical T stage (depth of invasion) (P<0.001), and clinical N stage (nodal) (P=0.018). Age, gender, tumor differentiation, Lauren's classification, and the presence of an ulcer were not found to be associated with adjacent organ involvement (P>0.05). When analyzed as a dichotomous variable with a cutoff value 407 mg/dl (3rd quartile), a fibrinogen level of >407 mg/dl was found to be strongly correlated with adjacent organ involvement (Chi-square test, P<0.001). Using the cutoff of 407 mg/dl, higher pre-operative fibrinogen level had a moderate specificity of 76.9%, and low sensitivity of 52.0% for predicting the presence of adjacent organ involvement. Table 4 shows a correlation between clinical stage and pre-operative fibrinogen level.
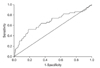
A receiver operating characteristics curve for preoperative fibrinogen level and the prediction of adjacent organ involvement is shown in Fig. 1; the area under the curve was 0.663. Adjacent organ involvement was observed in 4 of the 432 cT2 (0.9%) patients, in 35 of the 462 cT3 (5.6%) patients, and in 11 of the 29 cT4 (37.9%) patients (Fig. 1).
4. Multivariate logistic regression analysis and adjacent organ involvement
Table 5 presents the results of multivariate analysis for adjacent organ involvement. Tumor size (P=0.007), lymphatic invasion (P=0.026), clinical T stage (P=0.001) and pre-operative fibrinogen level (P=0.028) were all found to be significantly associated with adjacent organ involvement in clinically diagnosed AGC patients.
5. Survival and pre-operative fibrinogen levels
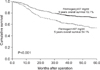
Patients were followed-up until death or until June 30, 2008. The median follow-up period for the 923 patients that remained alive at the cut-off date was 40 months. Fig. 2 shows the association between preoperative plasma fibrinogen level and overall survival. Higher levels of preoperative fibrinogen were found to be associated with a poorer prognosis by Kaplan-Meier analysis with the log-rank test (P<0.001).
Discussion
In the present study, we assessed pre-operative plasma fibrinogen levels in 923 patients with clinically diagnosed AGC and attempted to determine the correlation between fibrinogen levels and adjacent organ involvement. The main findings of this study were: 1) pre-operative plasma fibrinogen levels in AGC patients are associated with depth of invasion, lymphatic invasion, age, tumor size, and histology; 2) pre-operative fibrinogen levels are associated with adjacent organ involvement in clinically advanced gastric cancer; and 3) higher pre-operative plasma fibrinogen levels are associated with a poor prognosis.
Although no clear mechanism was identified, fibrinogen is known to be a major acute phase protein, and to be present in plasma at elevated levels in the presence of a malignancy or systemic inflammation.(7) Furthermore, fibrinogen levels are known to be associated with disease extent in esophageal cancer, non-small cell lung cancer, and others.(19,20)
Lymph node metastasis and depth of invasion are critical considerations when determining optimal treatment modalities in gastric cancer patients, and are also the most valuable prognostic factors.(21,22) The possibility of adjacent organ involvement is also an important consideration when deciding on resection in advanced gastric cancer, because it raises the issue of combined resection. In the present study, we found that pre-operative plasma fibrinogen levels were correlated with the presence of adjacent organ involvement in clinically AGC by univariate and multivariate analysis. The reason for the close correlation between elevated fibrinogen level and cancer metastasis might be that it enhances the sustained adherence of tumor cell emboli in the vasculature of target organs, resulting in the establishment of metastases.(23) To survive, metastatic cancer cells must leave the primary tumor, migrate into the lymphovascular system, and establish a new blood supply at their metastatic site.(24) The mechanism of the correlation between pre-operatively elevated fibrinogen levels and adjacent organ involvement was unclear. A possible explanation for tumor progression might be, that fibrinogen is known to be associated with tumor cell migration and formation of tumor stroma. For adjacent organ invasion tumor cells excrete lytic enzymes and consecutively are able to migrate.(24,25) This step of tumor cell movement might be associated with hyperfibrinogenemia.
The ability to assess adjacent organ involvement during or prior to surgery is important in terms of therapeutic decision-making. If gastric cancer has invaded adjacent organs, such as, the spleen, pancreas, colon, liver, or diaphragm, combined resection with a negative resection margin may be possible. However, combined resection has also been reported to be an independent predictor of a higher operative morbidity rate.(2,26) Accordingly, combined resection without adjacent organ involvement in an arbitrary situation increases the risk of surgical complications due to unnecessarily expansive surgery. Our findings suggest that preoperative fibrinogen level is an important consideration in clinically advanced gastric cancer, because it might help avoid unnecessary wide surgery. The relation found in the present study between poor overall survival and a higher preoperative fibrinogen level is consistent with that found by Yamashita et al.(10)
To the best of our knowledge, the present study is the first to suggest an association between pre-operative plasma fibrinogen levels and adjacent organ involvement. More limited surgery and adjuvant therapy might be indicated in patients with a higher fibrinogen level. Furthermore, the functional inhibition of fibrinogen might represent a novel therapeutic approach in AGC.
In the present study, pre-operative plasma fibrinogen was found to a useful clinically marker of adjacent organ involvement and overall survival. Moreover, when pre-operative fibrinogen is high, surgeons should consider adjacent organ involvement in clinically AGC patients. Finally, pre-operative fibrinogen may be a prognostic indicator in patients with gastric cancer.




 XML Download
XML Download