

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Mesenteric pseudocyst is a term used to describe abdominal cystic mass without the origin of abdominal organ.(1) This has been classified according to embryologic, ehiologic, histologic, and ther data, causing considerable confusion. It was considered the term mesenteric cyst as merely descriptive, and apply a histologic classification such as lymphangioma, pseudocyst, enteric duplication cyst, enteric cyst, and mesothelial cyst.(2) We presented a case of mesenteric pseudocyst of the small bowel in a 70-year-old man.
Case Report
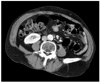
A 70-year-old man was referred to our hospital for operation of gastric cancer with a 1-month history of progressively worsening epigastric and intermittent peri-umbilical discomfort. He had no specific previous medical or surgical history including cancer. On physical examination, no tenderness or palpable mass were identified. Esophago-gastro-duodenoscopy (EGD) showed a 3.5 cm sized excavated lesion on the posterior wall of angle. Endocopic biopsy confirmed a histologic diagnosis of poorly differentiated adenocarcinoma including signet ring cell component. Endoscopic ultrasonography revealed invasion of caner to the proper muscle layer. Abdominal computed tomography (CT) scan showed a focal mucosal enhancement in posterior wall of angle of stomach, a 2.4 cm sized enhancing mass on distal small bowel loop without distant metastases or ascites in rectovesical pouch, and multiple gallbladder stones (Fig. 1). These physical, laboratory, and radiological findings prompted us to diagnose early gastric cancer, and gastrointestinal stromal tumor of small bowel. A pheripheral blood count showed no leukocytosis or anemia. Laboratory testing revealed alfa-fetoprotein level of 2.88 (normal range, 0 to 9 ng/ml), carcino-embryonic antigen level of 1.45 ng/ml (normal range, 0 to 5 ng/ml), carbohydrate antigen (CA) 19-9 level of 6.5 U/ml (normal range, 1 to 35 U/ml), and CA 72-4 level of 4.8 U/ml (normal range, 0 to 4 U/ml). Other laboratory test results were within normal limit.
The patient underwent subtotal gastrectomy with gastroduodenostomy, segmental resection of small bowel, and cholecystectomy. Mesenteric mass was adhered severely with greater omentum at the mesenteric side of small bowel, and mesenteric fat tissues. It looked like having connection with small bowel lumen. Small bowel, mesentery, and mesenteric mass were resected en-bloc methods, and end to end anastomosis was performed. After fixation of the surgical specimen, macroscopic examination revealed a uni-locular cyst measuring 3×3×2 cm in size. The mass contained yellow gelatinous materials with 1mm sized wall diameter. Pathological examination revealed 3 cm sized fibrous cystic wall without endothelial or epithelial lining and foam cell collection (Fig. 2, 3). The final pathological diagnosis was mesenteric pseudocyst. Pathologic stage of gastric cancer was T1bN1M0 (6th International Union Against Cancer TNM staging system); invasion to submusosa, metastases to 4 perigastric lymph nodes out of 16 retrieved nodes, and negative resection margin. Cholecystectomy specimen was reported as chronic cholecystitis with multiple gallbladder stones.
Discussion
Mesenteric pseudocysts are very rare intraabdominal mass with an incidence of about 1 case per 100,000 hospital admissions.(3) Ros et al.(2) first used the term "pseudocyst" in the classification of mesenteric cyst. Mesenteric pseudocyst could be located in the small bowel, large bowel mesentery and even retroperitoneum.(1,4) Most reports were pseudocyst of large bowel or retroperitoneum.(1) Although most mesenteric pseudocysts are asymptomatic, symptomatic mesenteric cysts could be associated with cyst size, cyst location, and complications, including infection, rupture, hemorrhage, and intestinal obstruction.(5) In our patient, there was no specific symptom associated with mesenteric pseudocyst except for intermittent vague periumbilical discomfort. If EGD and CT scan were not performed in this patient presenting non-specific abdominal pain, the diagnosis of mesenteric pseudocyst would be delayed.
To the best of our knowledge, this is the first case report describing incidentally detected mesenteric pseudocyst of small bowel in gastric cancer patients. When clinician performed staging work up for gastric cancer, should be aware the possibility of associated intraabdominal lesions.


 XML Download
XML Download