

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Gastric cancer (GC) is one of the most common cancers in Korea. According to the National Cancer Information Center of Korea, the incidence of GC in 2008 was 56.8 cases per million. Surgical resection is the treatment of choice for GC and curative (R0) resection of the tumor is the principal goal of surgery. This implies removing the tumor with sufficiently distant proximal and distal margins.
Microscopic resection margin involvement has been reported to affect poor prognosis in GC patients performed with resection.(1-3) Therefore, if the conditions of patient are tolerable and possible for more resection technically, it is recommended to achieve curative resection through a reoperation with more resection. Several studies had reported that the macroscopic and histopathological characteristics of the tumors were associated with the resection margin involvement.(1,4,5) Likewise, the frequency of resection margin involvement on the frozen section diagnosis would be considered as having relation to the specific clinical or histopathological characteristics of the tumors as well.
Generally, when performing gastrectomy to treat GC, a frozen section diagnosis is to be conducted on the resection margins in order to secure clear resection margins. The extent of resection is determined usually depending on tumor's location and gross type (Bormann's classification), and the final surgical procedure is determined depending on the resection margin involvement identified on the frozen section diagnosis. The macroscopic and histopathological characteristics of the tumor are examined through preoperative esophagogastroduodenoscopy (EGD) and biopsy. When the resection margin involvement-related characteristics are identified among them, it would be helpful for determining the extent of gastrectomy accordingly.
The purpose of this study is to make comparisons of the macroscopic and histopathological characteristics of the tumor as well as the prognosis depending on the resection margin involvement in the patients underwent gastrectomy for GC.
Materials and Methods
This study was conducted retrospectively in 83 margin-positive patients with GC on the frozen section diagnosis among the patients to whom the curative resection had been performed from July of 1995 to September of 2006 at the Samsung Medical Center.
Age, gender, types of operation and implementations of post-operative adjuvant chemotherapy or radiotherapy were examined by using the medical records and the size, location, macroscopic type, histological classification and the stage of the GC were examined by review of the histopathological findings.
Patients with multiple lesions were excluded on this study, and the size of tumor was measured based on the long axis of lesion. The locations of tumor were divided based on the center of the lesion into three parts of upper third, middle third and lower third. When the lesion was located spanning over two parts or more, such case was described as the diffuse GC. Depending on the location of tumor, the subtotal gastrectomy, proximal gastrectomy or total gastrectomy with D2 lymph node dissection had been performed. And the frozen section diagnosis was performed on the proximal and distal resection margins during operation in all patients. The patient with resection margin involvement on the frozen section diagnosis was performed additional resection during the operation. As the reconstruction, Billroth-I or Billroth-II anastomosis was performed in case of the subtotal gastrectomy while Roux-en-Y anastomosis was performed in case of the total gastrectomy.
After surgery, resection margin status and histopathological characteristics were identified by review of the final histopathological diagnosis. The counts of intra-operatively resected lymph nodes and the counts of metastatic lymph nodes had been analyzed, and the final stage of the cancer was operated in accordance with American Joint Committee on Cancer/Union Internationalis Contra Cancrum 7th staging system.(6)
For comparison with the patients who had shown as resection margin involvement on the frozen section diagnosis but achieved curative resection by more resection, the patients to whom curative resection could be achieved without more resection as not showing resection margin involvement on the frozen section diagnosis were selected as the control group. The control group was randomly selected on the patients whose age, gender, TNM stage and the status of adjuvant chemoradiotherapy equal to the patients of the study group among the patients undergone the curative gastrectomy in the same period. Also the clinical and histopathological characteristics were compared between the study group and the control group. And survival rate was analyzed in the two groups.
IBM SPSS ver. 19.0 (IBM, New York, NY, USA) was used for the statistical analysis. The stratified logistic regression analysis for univariate analysis and multivariate stratified logistic regression analysis were employed in the inter-group comparisons of clinical and histopathological characteristics. Kaplan-Meier survival analysis and stratified Cox regression analysis were used to calculate the survival functions. The P-value less than 0.05 was considered to indicate statistical significance.
Results
The mean age of 83 patients achieved curative resection with more resection as being identified as resection margin involvement on the frozen section diagnosis was 54.6 years old for 55 male patients (66.3%) and 28 female patients (33.7%). Mean follow up period was 50.9 months. The comparisons were made on the clinical and histopathological characteristics between two groups (Table 1).
The size of tumor was significantly larger in the study group than in the control group (7.7±4.4 cm vs. 5.8±3.0 cm; P=0.037). The patients of the study group had more number of tumors positioned at the lower third (55.4%), in contrast that the patients of the control group had more number of tumors positioned at the middle third (48.2%), presenting significant difference (P=0.003). Accordingly, the largest proportion of patients performed with the total gastrectomy was 79.5% in the margin-positive patients on the frozen section diagnosis. Whereas the largest proportion of patients performed with the subtotal gastrectomy was 62.7% in the margin-negative patients, presenting there were significant differences between two groups (P<0.001). All patients had undergone the gastrectomy with D2 lymph node dissection, and there was no inter-group difference in the counts of resected lymph nodes (P=0.868).
On macroscopic characteristics according to Bormann's classification, most of the lesions were in type-III and type-IV in both groups, but there was no inter-group difference (P=0.499). According to the World Health Organization histological classification, the patients of the study group had more of poorly differentiated type and signet ring cell type but there was no inter-group difference (P=0.126). Also on Lauren's classification, the most population in both groups was the diffuse type, yet the patients of the study group had less number of intestinal type tumors showing significant inter-group difference (20.5% vs. 34.9%; P=0.021). The distance of final proximal and distal resection margins had no inter-group difference (P=0.976, P=0.167).
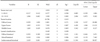
The results of the multivariate analysis, it only showed the location and Lauren's classification were the independent factors contributing to the resection margin involvement on the frozen section diagnosis (Table 2).
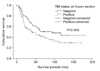
We performed the survival analysis, and showed the Kaplan-Meier survival curves with significant difference in both groups (P=0.049) (Fig. 1). The 5-years survival rates were 43.7% in study group and 53.9% in control group. The median survivals of each group were 41.0±11.5 months and 93.0±30.3 months, showing it was shorter in the study group. When the variables had been calculated through the stratified Cox regression analysis, it was examined that the TNM stage and resection margin status on the frozen section were identified as the key variables affecting the patient survival (Table 3).
Discussion
1. Determination of the extent of gastric resection
The extent of resection for curative gastrectomy is determined by the location and the size of lesion as well as by the distance of resection margins.(7,8) Even though there is no definitely established rule for the distance of resection margins, the treatment guidelines provided by the Japanese Gastric Cancer Association (JGCA) recommend to secure the distance ≥2 cm for T1 tumor, ≥3 cm for T2 or more deep tumor with expansive growth pattern and ≥5 cm for tumor with infiltrative growth pattern.(9) In determining the extent of resection according to these guidelines, usually there will be no objection to the extent of resection for the tumor located at upper third or lower third of stomach, but the extent of resection for the middle third tumor is controversial. Clark et al.(7) argues the total gastrectomy is required as the curative standard therapy for the GC located at the middle third, but other studies argue the subtotal gastrectomy is sufficient enough in consideration of post-operative complications or the quality of life because the extent of gastric resection and the distance of proximal resection margins do not have any effects on the long-term survival in contrast.(10,11) The surgeons in this study had determined the extent of resection by securing resection margins being recommended by the treatment guidelines provided by the JGCA depending on the results of pre-operative EGD and the computed tomography as well as the intra-operative gross findings.
2. Prognosis of patient identified with resection margin involvement on the frozen section diagnosis
The resection margin involvement after gastric surgery for GC has been known to act as the independent factor having negative effects on the prognosis.(3,4,8,12,13) Cascinu et al.(14) had reported that the resection margin involvement in the patient with N0 stage disease had effects on poor prognosis therefore reoperation was required, whereas in the patient being identified with metastatic lymph nodes would not have any prognostic differences caused by the resection margin involvement, it was possible to have close observation. Another similar study also had reported that the resection margin involvement was identified as independent factor having effects on poor prognosis only in the patients with ≤5 positive lymph nodes so that the survival had been affected more by the extent of lymph node metastases rather than the status of resection margin involvement.(15) But according to the recent studies, it was reported that the resection margin involvement had negative effects on the prognosis with no relation with lymph node metastases, being opened to dispute.(3,13)
Generally, a frozen section diagnosis of the resection margins is being performed during the surgery for GC to secure a clear resection margin. And through such diagnosis, if necessary, more resections are to be performed on margins during the surgery to achieve curative resection as possible as it can be. It should be noted that all of previous studies were performed in the patients identified with resection margin involvement from the results of the final histopathological diagnosis. This study is the first one conducted comparative analysis of the characteristics and the prognosis of patient in those who had achieved curative resection through having more resections among the patients with resection margin involvement on the frozen section diagnosis.
In this study, the patient who had achieved curative resection through more resection as identified with resection margin involvement on the frozen section diagnosis had shown comparatively lower survival rate than those with negative margins. Nevertheless, according to the results of multivatiate analysis, not only the TNM stage but also the resection margin status on the frozen section diagnosis was identified as factors affecting the survival. This result can be deemed that the resection margin involvement on the frozen section diagnosis was also likely to affect the survival likewise the resection margin status was identified as an independent factor with effects on the survival from previous studies performed in patients with microscopic residual disease determined by the final residual tumor status.
It is still unclear as far as the mechanism is concerned for how the resection margin involvement on the frozen section could have negative effects on the survival at the initial resection. When compared the distance from the lesion to the resection margins, there was no significant inter-group difference in both of proximal and distal resection margins, so that it could not be considered as the survival-affective factor (Proximal 4.4±4.2 cm vs. 4.4±3.0 cm, P=0.976; Distal 6.2±5.3 cm vs. 5.2±4.0 cm, P=0.167). The curative resection of tumor should be done with en-bloc resection of primary cancer ensuring there would be no microscopic or macroscopic residual tumor in principal. Although, there was no discussion on the patterns of recurrence in the patients, but it is presumable that those exposed tumor cells were exfoliated into abdominal cavity at the initial resection and affected the survival of margin-positive patients on the frozen section.
3. Characteristics of tumors with high prevalence of resection margin involvement
There are several studies concerning the patient prognosis and needs of additional treatments depending on the resection margin status after gastrectomy for GC. In these studies, reports are made that macroscopic Borrmann type III and IV, tumor size, tumor and nodal stage, tumor location, and histologically undifferentiated tumors are associated with resection margin involvement.(1,3,5) Since it is universalized to use the frozen section diagnosis in order to determine the extent of resection during gastrectomy, it can be applied to the tumors with resection margin involvement on the frozen section diagnosis in order to identify their clinical and histopathological characteristics. In this study, the status of resection margin involvement had shown differences according to the size, location of tumors and Lauren's classification, presenting similar results to the previous studies conducted in the patients with the resection margin involvement on the final diagnosis. It is considered that mid-third or upper-third location of the tumor and Lauren' s indeterminate histological type are predominant risk factors of resection margin involvement on the frozen section diagnosis.
This study has some limitations, due to the relatively small subject patients and the method of retrospective selection for the control group among those being performed with surgery in the same period. But the comparability was strengthened through random selections by matching age, gender, TNM stage of the patients and the status of adjuvant chemoradiotherapy.
In curative resection for GC, when the tumor was identified as located at mid-third or upper-third and in the case applicable to Lauren's indeterminate histological type, they are highly likely to show the resection margin involvement on the frozen section diagnosis and it can have negative effects on the prognosis. Therefore, it is considered that for tumors with these characteristics, it would be better to achieve en-bloc resection through more extensive resection than routine distance.


 XML Download
XML Download