

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Gastric cancer is one of the most common malignant tumors, and 5-year survival rate has been reported to be approximately 27-52%.(1,2) The overall prognosis is still poor, nonetheless, recently, the trend is that treatment outcomes are on the improvement due to early diagnosis and appropriate treatments.(2) The treatment methods and prognosis of gastric cancer are determined by the level of local infiltration of tumors, lymph node metastasis, and distant metastasis. As the detection rate of early gastric cancer is increased and to improve quality of life, endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD), laparoscopic gastrectomy, and other minimal invasive treatment methods are selected more. To determine such treatment methods, results of the studies that analyzed the role of endoscopic ultrasonography (EUS) have been reported.(3-5)
The Japanese Gastric Cancer Association (JGCA) has suggested early gastric cancer that is differentiated adenocarcinoma, tumor size is smaller than 2 cm, depth of invasion is limited to the mucosal layer, and without ulcerous changes and without lymph node metastasis as indication for endoscopic dissection.(6) In addition, cases who are diagnosed as stage 1 gastric cancer (T1N1M0, T2N0M0) by the preoperative diagnosis of disease stage are indications for laparoscopic gastrectomy.(7) In order to select appropriate minimal invasive treatments, accurate preoperative diagnosis of disease stage is essential. For the diagnosis of T disease stage, the accuracy of EUS is 78-93%, it is one of tests of which reliability is high, and its accuracy is higher than computed tomography (CT).(8,9) EUS is useful to distinguish T1m from T1sm, and T1 from T2 lesions. Nonetheless, the accuracy may be affected by endoscopic findings (microinfiltration of tumors, inflammatory changes in the vicinity of tumors, severe fibrosis associated with ulcers, benign ulcerous changes, benign cystic changes of the submucosal layer, deformity of the muscularis mucosa, insufficient tests, etc.), the location of lesions, the disease stage of gastric cancer, and research methods.(3,4,10)
In this study, the authors discuss whether EUS is an appropriate marker that determines treatment approach through the accurate diagnosis of disease stage by analyzing the accuracy of EUS as well as factors that exert effects on the accuracy of EUS for the preoperative diagnosis of local disease stage of early gastric cancer.
Materials and Methods
Selected among patients who underwent laparoscopic gastrectomy at the Ajou university hospital from February 2007 to January 2010, this study was conducted retrospectively on 152 patients who underwent EUS for the determination of local disease stage prior to surgery. At our hospital, when gastric cancer is definitely diagnosed by endoscopic examination and histological tests, EUS and CT are performed to determine clinical disease stages. In the year of 2003 when laparoscopic surgery was initiated, indication was limited to early gastric cancer. Recently, with the accumulation of experiences, the principle is to perform laparoscopic gastrectomy on cases whose T stage assessed by EUS is lower than T3, and N stage assessed by CT is lower than N1, excluding lesions that are indication of endoscopic resection suggested by the JGCA. By the analysis of the medical record of the subject patients, results of radiological tests, and results of histological tests, the level of the local infiltration of cancer, lymph node metastasis, and the accuracy of the preoperative evaluation of disease stage were examined. In addition, to examine the factors that exert effects on the accuracy of the preoperative evaluation of the diagnosis of disease stage, the accuracy of preoperative EUS evaluation according to tumor size, location, macroscopic morphology, and histological findings was compared and analyzed. The macroscopic morphology of tumors was evaluated according to the JGCA classification. It was defined that the elevated type was early gastric cancer type I, the depressed type was type III, the flat type was type II, and the mixed type was the combination of more than 2 types of the above basic types.(11) Histological findings were classified according to the classification of World Health Organization (WHO), and poorly differentiated adenocarcinoma, mucinous adenocarcinoma, and signet ring cell adenocarcinoma were classified as undifferentiated types.(12) The final disease stages that were analyzed by the results of histological tests were evaluated according to the tumor disease stage of the International Union against Cancer (UICC), 7th edition.(13)
1. Depth of invasion by EUS
EUS used in this study was the Ultrasound miniprobe UM-3R (ultrasound frequency 20 MHz, depth 4 cm, Olymphus, Tokyo, Japan). After the pretreatment identical to the upper gastrointestinal endoscopic tests, assessing lesions by endoscopes was performed. Operators were an identical team consisting of gastroenterologists with the experiences more than 50 cases of endoscopic ultrasonography annually, and it was performed under the supervision of a mentor professor. The stomach wall was divided to 5 layers and examined by EUS. The local infiltration level of lesions was evaluated by defining the sum of high echo of the first layer and the low echo of the 2nd layer as the mucosa (m), the high echo area of the 3rd layer as the submucosa (sm), the low echo area of the 4th layer as the muscularis propria (pm), and the high echo layer of the 5th layer as the subserosa (ss) and the serosa (s).
2. Surgical methods
According to the Japanese gastric cancer treatment guideline, D1+β lymph node resection was performed for T1N0M0 lesions, and D2 lymph node resection was performed for lesions higher than T2N0M0.(14) For cases with tumors in the upper stomach, total gastrectomy was performed. As reconstruction methods, for total gastrectomy cases, Roux en Y reconstruction was performed. For subtotal gastrectomy cases, Roux en Y, Billroth-I and Billroth-II reconstruction were performed.
3. Statistical analysis
For statistical analysis of the data, the SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA) was used. For the analysis of the association of clinical characteristics with the accuracy of EUS, univariate analysis was performed by chi-square test, and multivariate analysis was performed by binary logistic regression analysis. P-value lower than 0.05 was defined as statistically significant levels.
Results
1. Patients' feature, endoscopic gross type and endoscopic ultrasound finding
Characteristics of the subject patient groups and characteristics of the lesions are shown in Table 1. The mean age of patients was 58 years (27~77 years), the male was 100 patients and the female was 52 patients. The average tumor size was 2.5 cm (0.2~8.0 cm). In regard to the location of tumors, the upper stomach was 11 cases (7.2%), the middle area was 53 cases (34.9%), and the lower stomach was 88 cases (57.9%). Concerning gross morphology of tumors, the flat type (type II) was 94 cases (61.8%), which was most prevalent, the depressed type (type III) was 29 cases (19.1%), the mixed type was 25 cases (16.4%), and the elevated type (type I) was 4 cases (2.6%), which was least prevalent. Endoscopic ultrasonographic results were that sm lesion was 65 cases (42.8%), which was most prevalent, m lesion was 47 cases (30.9%), pm lesion was 26 cases (17.1%), and ss lesion was 14 cases (9.2%).
2. Surgical and pathologic results
In regard to gastrectomy methods, total gastrectomy was 9 cases (5.9%), subtotal gastrectomy was 142 cases (93.4%), and wedge resection was 1 case (0.7%) (Table 2). The 1 case who received wedge resection had a m lesion in the upper stomach in EUS, and endoscopic resection was performed. Nonetheless, after surgery, due to perforation, emergency laparotomy and wedge resection were performed, and pathological results were a sm lesion. Pathological findings of patients were that the differentiated type was 62 cases (40.8%), and the undifferentiated type was 89 cases (58.6%). Concerning T disease stages, T1 lesion was 119 cases (78.3%), and the lesion higher than T2 were 32 cases (21.0%). Histological findings could not be found in 1 case. The 1 case whose histological results could not be found was early gastric cancer in the middle anterior stomach wall, and by endoscopic histological tests, it was confirmed to be adenocarcinoma, and it was confirmed to be sm by EUS, and thus laparoscopic subtotal gastrectomy with billroth II gastrojejunostomy was performed. Nonetheless, in pathological findings, only ulcers were detected and residual cancer was not detected. The final disease stage of 132 cases (86.8%) was stage 1 gastric cancer.
3. Diagnosis of tumor depth by EUS comparing with pathologic results
In the entire 152 cases, cases whose EUS results concurring to pathological T disease stage were 63 cases (41.4%), underestimation was 32 cases (21.1%), and overestimation was 57 cases (37.5%). According to tumor size, in 46.8% of patients with tumors smaller than 3cm, EUS concurred to pathological results. Regarding cases larger than 3 cm, in only 27.9% cases, EUS concurred to pathological findings (P=0.033). In addition, in cases with tumors in the upper stomach or in the distal stomach, the concurrence rate of EUS was shown to be lower than the body area cases, nonetheless, statistical significances were not shown (P=0.096). When analyzed according to macroscopic morphology, regarding the depressed type, only in 24.1% cases, it concurred to pathological findings, and thus it was statistically significant (P=0.035). On the other hand, in the analysis of the concurrence rate of EUS to pathological results according to histological findings, the differentiated type was 33.9%, the undifferentiated type was 47.2%, and statistically significant differences were not shown (P=0.102) (Table 3). In multivariate analysis, tumors located in the upper stomach (P=0.035) and tumors of which macroscopic morphology was the depressed type (P=0.029) were shown to be factors that could predict the discordance of EUS to histological findings, and particularly, cases with depressed macroscopic morphology were the most significant factor (OR=2.873) (Table 4).
4. Overestimate and underestimate by EUS
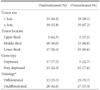
When cases with the inaccurate evaluation of tumor infiltration by EUS were analyzed, in cases that tumors were located in the upper stomach, 62.5% cases were underestimated. In cases with non-depressed macroscopic morphology, 77.6% cases were underestimated. On the other hand, when tumors were located in the body area or the lower area, 60.0% and 69.6%, respectively, were overestimated. In cases with non-depressed macroscopic morphology, 77.6% cases were overestimated. In cases that histological findings were the differentiated type, 70.7% cases were overestimated (Table 5).
Discussion
In Asia including Korea and Japan, the rate of the early diagnosis of gastric cancer becomes high, and with the increased ratio of patients older than 70 years whose postoperative complications and mortality rate are relatively high, endoscopic treatments for gastric cancer or minimal invasive treatments such as laparoscopic surgery became common procedure.(5,15) In gastric cancer, lymph node metastasis is determined by tumor infiltration levels, and thus for such minimal invasive treatments, differentiation of T1m from T1sm, and differentiation of T1 from T2 lesion are important.(3) In the past, local infiltration levels were evaluated by clinical findings, CT, magnetic resonance imaging (MRI), etc., nonetheless, their accuracy is not high.(2,3) EUS examines the stomach wall by dividing each layer and thus it could evaluate the level of tumor infiltration more accurately. Hence, in the preoperative diagnosis of disease stage of gastric cancer, attentions have been focused on the accuracy and usefulness of EUS, and several studies have reported that EUS is useful for the diagnosis of local disease stage of gastric cancer.(2,4,5,16) EUS diagnoses the T stage of tumors depending on the depth of infiltration that destroys the normal layer structure of stomach wall by the low echo irregular mass findings.(17) Although it is different depending on the literature, for the diagnosis of the T stage of gastric cancer, the accuracy of EUS has been reported to be 65-92%, and it may be influenced by several factors.(4) In our study, in the evaluation of the local infiltration level of tumors, the accuracy of EUS was 41.4%, and EUS was performed by surgeons with abundant experiences, nonetheless, it was shown to be lower than the studies that have been reported until now. Until now, most clinical studies that examined the accuracy of EUS were conducted exclusively on the specific part of depth of invasion or studies that analyzed the accuracy on T stages.(4,5,16,17) It could be anticipated that in our study, it was analyzed including all types of infiltration depth that could be classified, and thus lower concurrence rates were shown in comparison with past studies.
Kim et al.(18) have reported that in cases with tumors of which macroscopic morphology was depressed type, cases associated with ulcer, or cases of which histological findings were undifferentiated, the accuracy of EUS was lowered, nonetheless, tumor size or location did not exert effects on the accuracy of EUS. On the other hand, Kim(3) have reported that in regard to the size of lesion, the accuracy of EUS was decreased in cases with lesions larger than 3 cm. Tsuzuki et al.(4) have reported that in cases with tumors located in the upper stomach, the accuracy of EUS was decreased significantly, nonetheless, the accuracy of EUS in the differentiated type and the undifferentiated type were not different. Tsuzuki et al.(4) have reported that in the entire 104 patients who underwent EUS prior to surgery, the accuracy of EUS was 86%, EUS underestimated the cases with lesions located in the upper stomach, overestimated lesions in the lower stomach, and underestimated the surface depressed type.
In our study, in univariate analysis, factors that exerted effects on the accuracy of EUS were tumor size, location, and macroscopic morphology. In multivariate analysis, tumor location and macroscopic morphology were analyzed to be significant factors, and results similar to the studies that were reported until now were shown. In regard to tumors located in the upper stomach, it was underestimated more than overestimated (62.5% vs. 37.5%), which is determined to be due to that as stated in previously reported studies, the submucosa of upper stomach is relatively thin, and due to fibrosis or blood vessels, infiltration to the submucosa may not be detected.(4) Lesions of which macroscopic morphology is the depressed type, most of them may be associated with ulcerous changes, and thus it is underestimated more than the elevated type or the flat type.(18)
It has been reported that the accuracy of EUS is lowered in undifferentiated adenocarcinoma. Kim et al. have reported that the accuracy of EUS was significantly reduced in undifferentiated cases, and it showed a tendency to underestimate.(19) However, in our study, a trend that the accuracy of EUS for differentiated lesions was lower than undifferentiated lesions was shown, nonetheless, it was analyzed to be not significant statistically, and it is required to analyze more cases. Based on the results, it could be concluded that based on endoscopic findings, cases with lesions located in the upper area and cases with depressed macroscopic morphology, even if they are indication for endoscopic resection, appropriate treatment methods should be selected carefully considering the possibility that it may be underestimated by EUS.
Of course, the analysis of the accuracy according to infiltration levels may be of help to select surgical methods, and thus its additional analysis may be of help. Nevertheless, the number of patients included in our study is too small to perform such analysis. In addition, all patients included in our study were patients who underwent laparoscopic surgery for gastric cancer, and most patients had relatively early lesions that were not indication for endoscopic resection. Although prediction factors for concurrence were found by multivariate analysis in our study, it is considered if studies on a large number of gastric cancer patients with diverse disease stages are conducted in the future, it would be of help to conduct studies on the significance of EUS for the selection of treatment methods as well as to analyze the results of EUS. In addition, in our institution, preoperative assessment of lymph node metastasis has been performed by CT, nevertheless, EUS is valuable for the assessment of lymph node metastasis in the vicinity of the stomach, and thus it is considered that its clinical studies are required in the future.
In gastric cancer, for the selection of treatment methods such as endoscopic resection, surgical treatments, the accurate diagnosis of disease stage prior to surgery is very important. In our study, in 152 patients who underwent laparoscopic gastrectomy for gastric cancer, preoperative EUS findings and postoperative histological findings were compared. It was analyzed that in cases with tumors located in the upper area and the morphological type was depressed type, the accuracy of EUS was low, and results similar to other investigators were obtained. Therefore, in cases with gastric cancer in the upper stomach and the depressed type, when endoscopic resection is considered based on EUS findings, it should be decided more carefully.




 XML Download
XML Download