

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
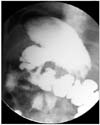
Because of advancement of medical treatment, surgical management of gastric or duodenal ulcer was indicated for treatment of perforation, massive hemorrhage and obstruction. The distal gastrectomy including ulcer was known as principle method of duodenal ulcer obstruction, but actually many surgeons have performed only bypass surgery for the difficulty of formation of duodenal stump. In our case, 61-year-old male with repetitive duodenal ulcer obstruction transferred with obstruction due to deformities and inflammations of duodenal ulcer. We had performed totally laparoscopic distal gastrectomy with ROUX-EN-Y reconstruction using the clear visibility of laparoscopy and fine dissections of harmonic scalpel. The patient started soft diet on postoperative day 5 and discharged on postoperative day 8. He returned to work after discharging immediately.
Figures and Tables



References
1. Andersen IB, Bonnevie O, Jorgensen T, Sorensen TI. Time trends for peptic ulcer disease in Denmark, 1981-1993. Analysis of hospitalization register and mortality data. Scand J Gastroenterol. 1998. 33:260–266.

2. Kang JY, Elders A, Majeed A, Maxwell JD, Bardhan KD. Recent trends in hospital admissions and mortality rates for peptic ulcer in Scotland 1982-2002. Aliment Pharmacol Ther. 2006. 24:65–79.
3. Kurata JH, Corboy ED. Current peptic ulcer time trends. An epidemiological profile. J Clin Gastroenterol. 1988. 10:259–268.
4. Ohmann C, Imhof M, Ruppert C, Janzik U, Vogt C, Frieling T, et al. Time-trends in the epidemiology of peptic ulcer bleeding. Scand J Gastroenterol. 2005. 40:914–920.
5. Datsis AC, Rogdakis A, Kekelos S, Zografos K, Sarantopoulou A, Spilliotis J. Simple closure of chronic duodenal ulcer perforation in the era of Helicobacter pylori: an old procedure, today's solution. Hepatogastroenterology. 2003. 50:1396–1398.
6. Kauffman GL Jr. Duodenal ulcer disease: treatment by surgery, antibiotics, or both. Adv Surg. 2000. 34:121–135.
7. Ng EK, Lam YH, Sung JJ, Yung MY, To KF, Chan AC, et al. Eradication of Helicobacter pylori prevents recurrence of ulcer after simple closure of duodenal ulcer perforation: randomized controlled trial. Ann Surg. 2000. 231:153–158.
8. Lee JH, Yang SJ, Jeong YW, Park SH, Kim JH, Park JM. Surgical treatment for chronic peptic ulcer with gastric outlet obstruction. J Korean Gastric Cancer Assoc. 2008. 8:160–165.
9. Lau WY, Leung KL, Zhu XL, Lam YH, Chung SC, Li AK. Laparoscopic repair of perforated peptic ulcer. Br J Sur. 1995. 82:814–816.
10. Robertson GS, Wemyss-Holden SA, Maddern GJ. Laparoscopic repair of perforated peptic ulcer. The role of laparoscpy in generalized peritonitis. Ann R Coll Surg Engl. 2000. 82:6–10.
11. Hallgrimsson P, Lovén L, Westerdahl J, Bergenfelz A. Use of the harmonic scalpel versus conventional haemostatic techniques in patients with grave disease undergoing total thyroidectomy: a prospective randomized controlled trial. Langenbecks Arch Surg. 2008. 393:675–680.
12. Adachi Y, Shiraishi N, Shiromizu A, Bandoh T, Aramaki M, Kitano S. Laparoscopy-assisted billroth i gastrectomy compared with conventional open gastrectomy. Arch Surg. 2000. 135:806–810.
13. Kim YW, Baik YH, Yun YH, Nam BH, Kim DH, Choi LJ, et al. Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: results of a prospective randomized clinical trial. Ann Surg. 2008. 248:721–727.
14. Lee JH, Han HS, Lee JH. A prospective randomized study comparing open vs laparoscopy-assisted distal gastrectomy in early gastric cancer: early results. Surg Endosc. 2005. 19:168–173.
15. Kim JH, Jung YS, Kim BS, Jeong O, Lim JT, Yook JH, et al. Learning curve of a laparoscopy assisted distal gastrectomy for a surgeon expert in performing a conventional open gastrectomy. J Korean Gastric Cancer Assoc. 2006. 6:167–172.
 XML Download
XML Download