

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Regional incidences of gastric cancer are variable, and the prevalence of the disease shows a declining tendency. However, gastric cancer remains the fourth most common malignancy worldwide, and there is a higher incidence of the disease in Far Eastern Asian countries, such as Korea and Japan.(1) This is in contrast to Western countries where the incidence is much lower. However, the West has relatively higher proportions of UTG compared with Asian countries.(2) Some recent studies have reported an increasing trend in the incidence of UTG in Japan, China, and Korea.(3-6) The 2004 Nationwide Gastric Cancer Registry also reported similar findings.(7) Such increases could be related to recent changes in lifestyles of the Korean population. Some studies in both Western and Eastern countries have reported a poorer prognosis with UTG.(8,9) Others, however, found that the prognosis of patients with UTG was no poorer than that of patients with MLG in each equal TNM stage. (10,11) It remains unclear whether the disease prognosis is due to different biologic characteristics or late detection. In this study, we evaluated chronological changes in the prevalence of UTG, the prognosis of UTG patients who underwent gastric resection at SNUH during the last 21 years, and potential prognostic indicators of UTG.
Materials and Methods
We retrospectively analyzed the medical records of 12,300 gastric cancer patients who underwent gastric resection between 1986 and 2006 at SNUH. The location of the tumor was defined according to a Standardized Pathology Reports Guideline for Gastric Cancer in Korea.(12) Patients were grouped based on the presence of UTG or MLG. Patients who had received neoadjuvant chemotherapy or who had remnant or recurrent gastric cancer, synchronous gastric cancer, any other primary malignancy, or gastric cancer involving the entire stomach were excluded from the study. We evaluated numeric and proportional changes in UTG characteristics by linear regression. We compared patient demographic variables between groups, such as age and sex and surgical variables including type of operation, operative radicalities, and survival rates. We also evaluated the status of lymph node metastasis, depth of tumor invasion, and TNM stage and assessed the tumors according to both the WHO's and Lauren's classifications. According to the WHO classification, the overall group was divided into an undifferentiated subgroup and a differentiated subgroup. The undifferentiated group included poorly differentiated cell types and signet ring cell types, and the differentiated group included well differentiated cell types and moderately differentiated cell types; papillary carcinoma and mucinous carcinoma were excluded from this subclassification.(13-15) To compare the prognosis, the 5-year survival rate was estimated in each group according to the TNM classification of the UICC 6th, and prognostic indicators in all patients, including tumor locations, were evaluated by univariate and multivariate analysis.(16) Cross-table analysis with Chi-Square tests and Independent-samples T test with Levene's test for equality of variances were used to compare each group, and missing values were excluded from statistical analysis in cell differentiation and Lauren's classification category, and the Kaplan-Meier method was used to estimate the survival rates by performing a log-rank test. A Cox-proportional hazard model was used in the multivariate analysis. All tests were two-sided and performed at the 5% level of significance using SPSS Statistics 17.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
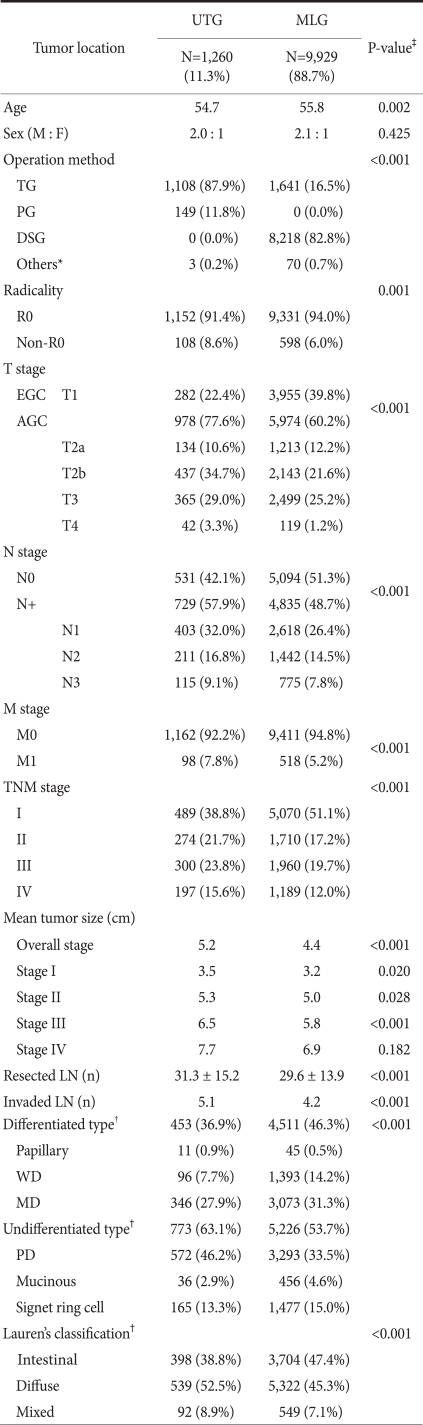
Among the 12,300 study group, 1,111 patients were excluded due to pre-operative chemotherapy (N=39), remnant gastric cancer (N=154), recurrent cancer (N=59), synchronous gastric cancers (N=457), synchronous other malignancy (N=55), gastric cancer involving the entire stomach (N=346), leaving a final study group of 11,189. The clinicopathological characteristics of these patients are shown in Table 1. The number of patients in the UTG group was 1,260 (11.3%), and the mean age was 54.7 years. The male to female ratio was about 2 : 1, which is not different from the MLG group. The proportion of patients with advanced gastric cancer was significantly higher in the UTG group compared with the MLG group (77.7% vs. 60.4%). Total gastrectomy was the most frequent type of operation performed in the UTG group; proximal gastrectomy was performed in 11.8% of the patients. The proportion of R0 resection was slightly lower in the UTG group compared with the MLG group (91.4% vs. 94%). The distribution of the TNM stage showed more advanced stage cancer in UTG than in MLG patients, and the mean number of cancer-positive lymph nodes was greater in the UTG group. The mean tumor size in the UTG group was larger than that in the MLG group (5.2 cm vs. 4.4 cm). When TNM stages were compared, the UTG group showed a significantly larger tumor size than the MLG group in all TNM stages except stage IV. There were some missing values in the cell differentiation and Lauren's classification categories due to limitations in medical records but the UTG group exhibited a significantly higher proportion of diffuse Lauren's type and a higher proportion of undifferentiated cell types compared to the MLG group (Table 1).
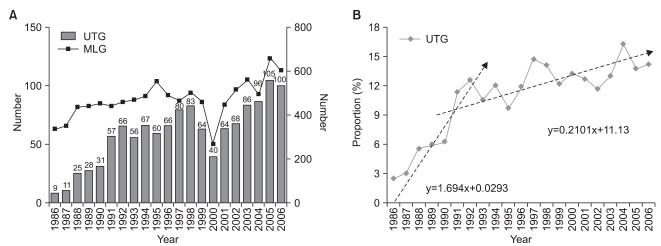
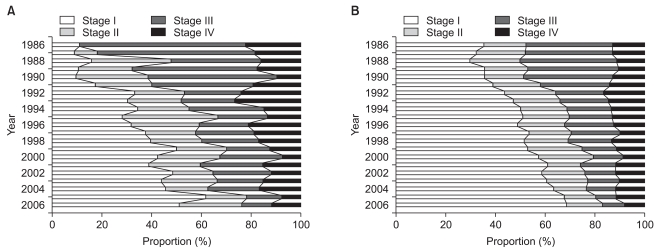
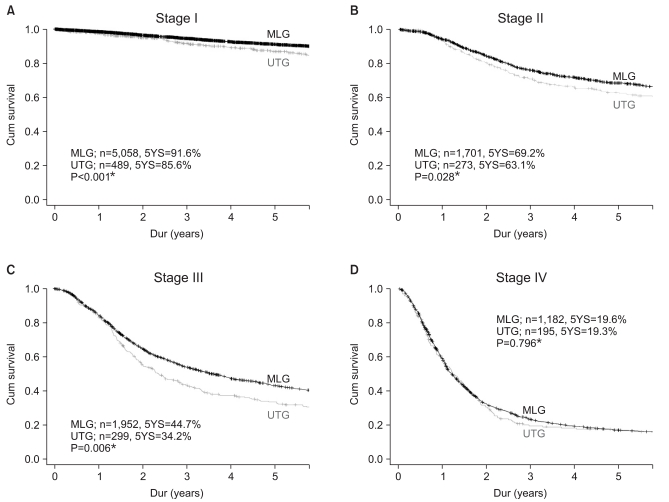
Chronologically, the proportion of UTG was 2.6% in 1986 and rapidly increased to 12.5% in 1992. Subsequently, the disease showed a slow increase, rising to 14.2% in 2006. The increase in the rate of UTG was estimated to be about 1.6% per year before 1992 (P<0.001); however, this dropped to 0.21% per year after 1992 (P=0.028) (Fig. 1). The median age for UTG was in the sixth decade of life from 1986 to 1995. This shifted to the seventh decade of life after 1996, a finding that was also observed in the MLG group. A chronological review of the TNM stage showed that stage I and II cancers were more prevalent in both the UTG and MLG groups than in the past (Fig. 2). Comparison of the individual stratified TNM stages showed that the 5-year survival rate of the UTG group was significantly poorer than that of the MLG in stage I-III (Fig. 3).
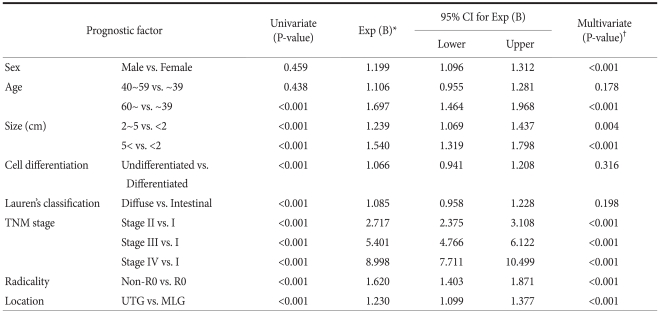
Tumor size, tumor location, Lauren's classification, cell differentiation, radicality, and TNM stage were identified as prognostic factors in univariate analysis. However, in multivariate analysis, sex, tumor size, tumor location, radicality, and TNM stage were found to be independent prognostic indicators (Table 2).
Discussion
The aim of this study was to evaluate chronological changes in the proportion of UTG during the past 21 years and to determine the prognosis of patients with UTG. In contrast to previous reports of an increasing trend in UTG worldwide, we found that the UTG proportions are nearly not changing these days. Prior to 1992, the prevalence of UTG showed a relatively rapid rise, with rates increasing up to 1.69% annually. However, this rate has decreased to 0.21% per year since 1992 at SNUH (Fig. 1). Those changes are not likely the result in real incidence but may be attributable to increasing rates of screening for early gastric cancer (EGC); there was a simultaneous increase in the proportion of EGC identified during the same period. The changes may also be due to patient characteristics, with specific types of patients being referred to the SNUH. According to a nationwide survey of gastric cancer in Korea in 2004, the prevalence of UTG had increased from 11.2% to 14.2%.(17) However, another nationwide survey of the disease in 2009 reported a UTG prevalence of just 13.4% in Korea and concluded that the increasing trend of UTG in Western countries has not been seen in Korea, a finding consistent with our study.(18) We observed a shift in the peak age distribution of UTG from the sixth to the seventh decade of life, which may be explained by the aging population in Korea. The decrease that we observed in TNM stage III and IV patients and the increase in stage I and II compared to the prevalence in the past could be attributable to technical advances in endoscopy and increased diagnosis of patients with early stage disease (Fig. 2).
In the prognosis analysis, patients with UTG showed a poorer prognosis than those with MLG, with significantly lower 5-year survival rates in each TNM stage, except stage IV. The poor prognosis with UTG compared with MLG may be due to a number of factors. There was significantly less EGC but higher numbers of advanced gastric cancer (AGC) in the UTG group compared with the MLG group; stage III and IV lesions were 39.4% and 31.7% in the UTG and MLG groups, respectively. A significantly larger mean tumor size in TNM stage I, II, and III, larger mean number of invaded lymph node, lesser operative R0 resection rates were observed in the UTG group (Table 1). In relation to lymph node metastasis, the main lymphatic channels could be different in each group, raising the possibility that the lymphatic system may be implicated in the poorer prognosis. Kunisaki et al.(11) previously reported that UTG metastases operating through the complex lymphatic systems such as lymphatic systems of the lower esophagus arising from the mediastinum, intraabdominal superior lymphatic systems to the pancreas, and retroperitoneal lymphatic systems from around the aorta all contribute to the prognosis of UTG. Thus, meticulous lymph node dissection is essential. An additional factor that may contribute to a poor prognosis according to Sasako et al.(19) is incomplete mediastinal lymph node dissection, which may occur due to technical difficulties from the abdominal approach. However, randomized controlled studies found no survival benefit with a thoracic approach for lower esophageal lymph node dissection; they also reported additional complications associated with this procedure. Unfortunately, we were unable to analyze any additional influence of either the lymphatic channels or lymph node dissection in patient prognoses due to limited data.
The anatomical nature of the upper third part of the stomach, which is somewhat different to the distal section, may also be implicated in a poor prognosis. According to Piso et al.,(20) the fact that the serosa layer is incompletely formed in the upper third section of the stomach may result in AGC (advanced gastric cancer) being more prevalent in UTG.
Thus, the poor prognosis of UTG may be related to various factors, such as stomach anatomy, very complex lymphatic systems, or technical difficulties during surgery. However, the tumor itself may also be different in UTG compared with MLG. In one analysis, UTG showed a significantly higher incidence of undifferentiated cell types than MLG, a finding consistent with other studies. Maeda et al.(21) reported that UTG had a more aggressive disease course and poorer prognosis due to undifferentiated or poorly differentiated cancer cells leading to advanced gastric cancer. In Lauren's classifications, UTG showed a higher proportion of diffuse type cells, whereas MLG exhibited more intestinal type cells (Table 1), all of which may be related to the differences in the pathophysiology of UTG and MLG. KcColl et al.(22) proposed that at least two different etiological mechanisms could underlie the prognosis in gastric cancer. One involved Helicobacter pylori infection or autoimmune atrophic gastritis in MLG; the other involved gastroesophageal reflux and nitric oxide production in saliva leading to the development of intestinal metaplasia, neoplasm, and more undifferentiated tumor cells in UTG. Thus, the upper third stomach differs from the middle and lower third stomach not only in anatomy but also in cancer development mechanisms.(23,24)
Many studies of UTG cite late detection as an important factor in the poor prognosis of the disease; the most common symptoms of UTG, such as weight loss and gastroesophageal reflux are usually very insidious and do not occur until the disease is at an advanced stage.(8,21,25) Some studies have argued that early detection can improve the prognosis if radical resection can be performed.(5,10,11) In our study, early stage UTG showed nearly a 90% 5-year survival rate, suggesting that more effort should be expended on the early detection and treatment of upper third gastric lesions. As noted previously by Yokoi et al.,(26) there are some limitations associated with UTG screening, such as the presence of trivial mucosal lesions, simple color changes, and technical difficulties. To ensure that UTG lesions are not overlooked, the endoscopist should pay special attention when examining lesions in the upper third stomach.
As this was a retrospective analysis and patients who did not undergo surgery because of advanced disease were not included, our study does not represent all the clinical aspects of UTG in Korea. However, from a surgical perspective, it may offer useful information.
In conclusion, the prevalence of UTG showed a temporary increasing trend prior to the 1990s, with an annual rise of 1.69%. However, since then, the annual rate of increase has been just 0.21% at SNUH. The UTG group showed significantly poorer 5-year survival rates compared with the MLG group in each TNM stage except stage IV. Tumor size, tumor location, radicality, and TNM stage were independent prognostic indicators in both univariate and multivariate analysis.
 XML Download
XML Download