

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Adverse drug reactions (ADRs) are considered a major international clinical concern and a significant cause of death in medical facilities [1]. It recommended that safer medical systems be developed to enable the early discovery of drug side-effects [23]. Although a voluntary reporting policy has been implemented to reduce ADRs, relatively few side-effects of drugs have been reported when compared to the actual number of incidents of adverse drug effects [4].
In the past, the occurrence of ADRs after the use of prescription drugs could be detected when the patients and doctors noticed adverse symptoms. Recently, many studies have attempted to detect ADRs using Electronic Medical Record (EMR) data [5]. Since the conversion of conventional paper-based health record systems to EMR systems, a considerable amount of medical information has been collected. Accordingly, diverse efforts have continued to systematically identify adverse drug effects without depending on voluntary reports. The large, computerized clinical databases associated with EMR can be used with various ADR detection methods. Moreover, they can serve as a source of information that clinicians can use to readily and appropriately respond in the event a patient suffers from an ADR [6].
In this study, we created an algorithm to enable early detection of ADRs using EMR data. We selected a 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMG-CoA reductase) inhibitor (HMG-CoA reductase inhibitor, which is a statin). A statin is a representative drug for the treatment of hyperlipidemia [78]. It facilitates both the primary and secondary prevention of cardiovascular disease by lowering low-density lipoprotein cholesterol [9]. However, statins cause various ADRs, such as myopathy, hepatotoxicity, nephrotoxicity, and insulin resistance disorder [1011]. Statin ADRs should be considered on a case-by-case basis because they are distinguished according to their specific metabolic pathways or drug interactions.
To improve the safety of patients who use statins, we developed an algorithm for automatically detecting liver injury due to statin use from EMR data, including coexisting diseases, laboratory findings, and concomitant drugs. To verify the algorithm's performance, a primary ADR analysis of the algorithm was performed after extraction of data of patients who were prescribed statins. A secondary chart review analysis was conducted. After comparing the primary algorithm assessment and secondary chart review analyses, we identified approaches to improving the algorithm's performance.
Go to : 
II. Methods
1. Study Subjects
In this study, we used EMR data from Seoul St. Mary's Hospital in Korea. The subjects of the study were patients who had been prescribed a statin for the first time among all outpatients of the hospital between January 2009 and December 2012. We defined liver injury due to statin use by a rise in either the alanine transaminase (ALT) level, specifically more than three times the upper limit of normal (ULN), or the alkaline phosphatase (ALP) level, specifically more than twice the ULN [12]. If there was no laboratory finding, such as ALT or ALP level, prior to statin prescription, we excluded those patients from the study. Seven types of statins (atorvastatin, fluvastatin, pitavastatin, pravastatin, rosuvastatin, simvastatin, and simvastatin plus ezetimibe complex) were investigated in our study.
2. EMR Data Extraction for Proposed Algorithm Development
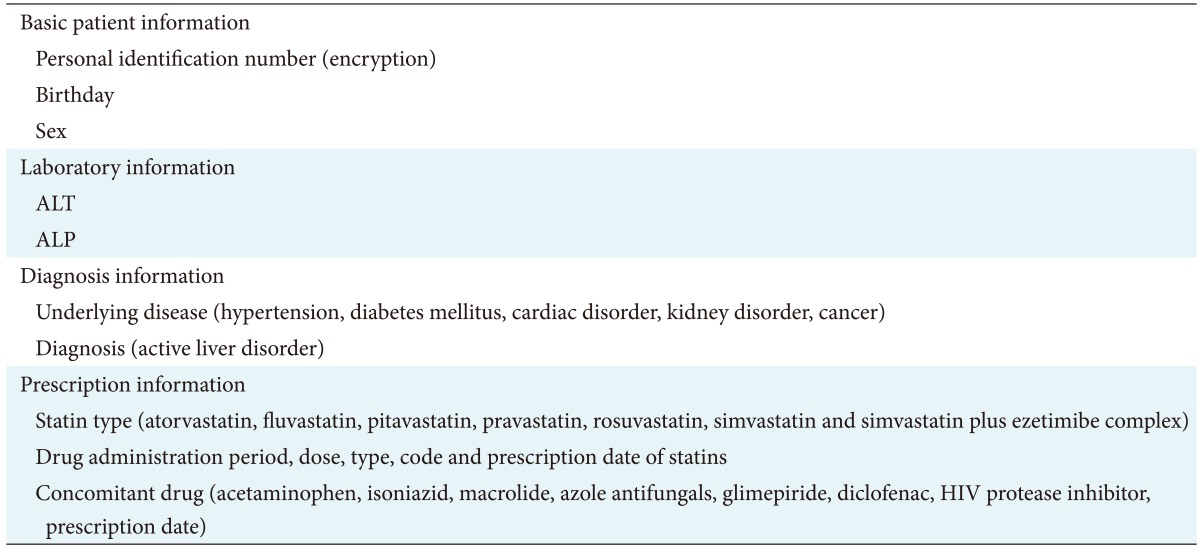
We extracted basic patient information, including patient identification number, date of birth, and sex. We additionally extracted the laboratory information of ALT and ALP levels every 3 months and on the date of the test. We extracted prescription information, including administration period, dose, type, code, and prescription date. We extracted any underlying disease, such as hypertension or diabetes mellitus. Furthermore, we extracted diagnosis information about active liver disease, such as viral hepatitis (International Classification of Diseases [ICD] B15–B19), malignant neoplasm of the liver, and intrahepatic bile ducts (ICD C22), and diseases of the liver (ICD K70–K77) within 1 year prior to statin prescription because the liver function test was abnormal. Lastly, we extracted concomitant drugs that may induce liver toxicity related to statin use. Some drugs have liver toxicity such as acetaminophen, isoniazid, macrolide, glimepiride, diclofenac, and so on [13] (Table 1).
3. Standard of ADR Assessment by the Proposed Algorithm and Chart Review
We conducted chart reviews regarding cases in which ADRs were suspected according to the ADR algorithm. We validated the algorithm results through a chart review. Experienced hospital doctors reviewed the medical charts of patients who were determined by the algorithm to be unlikely to have an ADR. The World Health Organization-the Uppsala Monitoring Centre (WHO-UMC) causality categories were used to assess the causal relationship between statin use and ADR and to ensure the assessment objectivity[14]. One of the doctors assessed the ADRs by assigning one of three criteria–‘Certain’, ‘Probable/Likely’, or ‘Possible’–based on a standardized protocol. The doctor discussed the ADRs and criteria with the other researchers for the ultimate assessment. If the algorithm and chart review results were different, we analyzed the cause for the difference. The performance of the algorithm was verified through a positive predictive value (PPV).
4. Privacy Protection
All patient data were encoded when extracted from the EMR. Only one of the main researchers had access to all the data. When the need arose for a statistical analysis or another task, patient-identifying information, such as registration number and name was deleted, and a unique random number was used instead. When a chart review by a doctor was required, data were provided to the doctor after re-identification, and the data were deleted after the assessment was finished. The study only used the data of patients who had completed treatment. Thus, by encoding the data and ensuring anonymity, patient rights and physical conditions were not affected. Therefore, informed consent was not required. Our study was approved by the Institutional Review Board of the Catholic University of Korea (No. MC12RNS10126).
5. Statistical Analysis
Descriptive statistics were presented as frequencies (%) of participants. To compare the statin type and statin-induced hepatotoxicity, the chi-square test or exact test were used. Analyses were performed with the use of SAS software ver. 9.4 (SAS Institute Inc., Cary, NC, USA) and two-sided p <0.05 was considered statistically significant.
Go to :
III. Results
1. Development of ADR Automatic Assessment Algorithm
We developed the algorithm to assess ADR occurrences based on the following four steps (Figure 1).
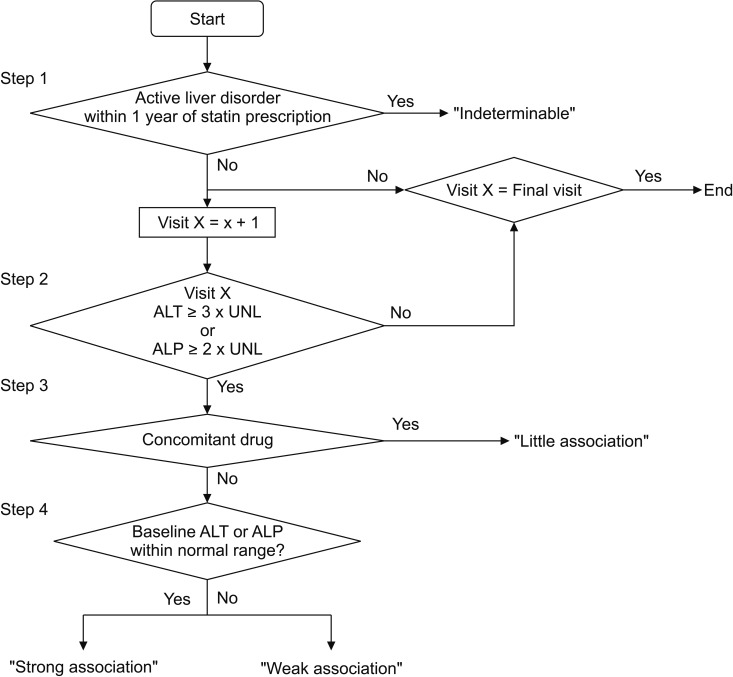 | Figure 1Algorithm of statin-induced liver injury assessment active liver disorder. Active liver disorder (International Classification of Diseases [ICD] B15–19), viral hepatitis (ICD C22), malignant neoplasm of the liver and intrahepatic bile ducts (ICD K70–77) diseases of the liver. Normal record of liver function tests: ALT 9–45 IU/L, ALP 30–120 IU/L. ALT: alanine transaminase, ALP: alkaline phosphatase, UNL: upper normal limits.
|
Step 1: Patients who had been diagnosed with active liver disorder within 1 year of statin prescription at the baseline were defined as ‘Indeterminable’.
Step 2: The record of ALT or ALP was monitored for patients and each visit. The ALT level was <3 × UNL or ALP level <2 × UNL. It was considered ADR-free and a recheck was conducted at a follow-up visit.
Step 3: Once the ALT levels ≥3 × UNL or ALP levels ≥2 × UNL were determined, the patients were examined to determine whether they were using concomitant drugs. If they were using concomitant drugs, they were classified as Little-association (Litt_AS).
Step 4: If the patients were not taking concomitant drugs, the baseline ALT and APL levels were checked. If these levels were within the normal range, the corresponding patient was classified as Strong-association (Str_AS). If not, the corresponding patient was classified as Weak-association (Weak_AS). The algorithm was looped for all patients through the end of the study.
2. Application of the Algorithm
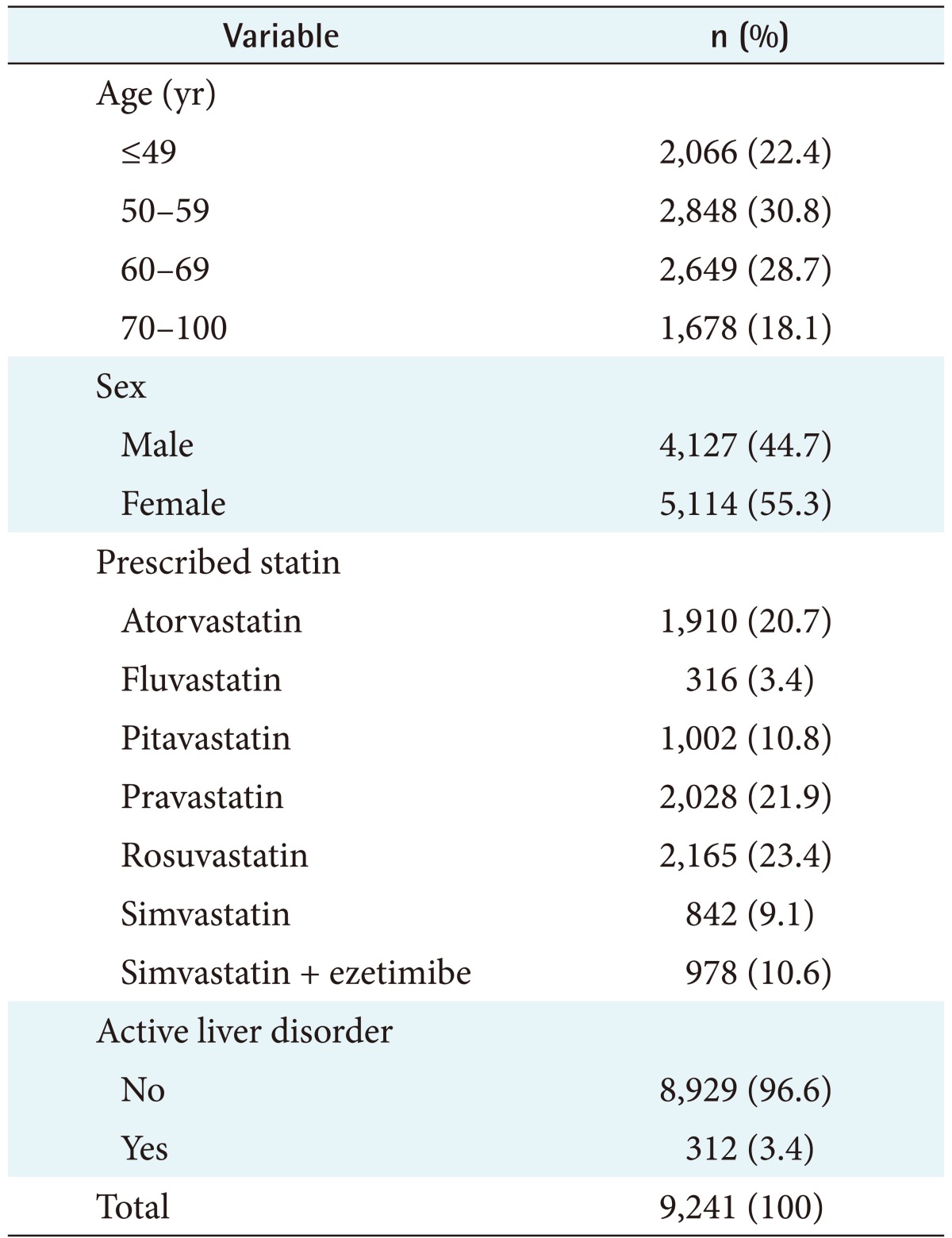
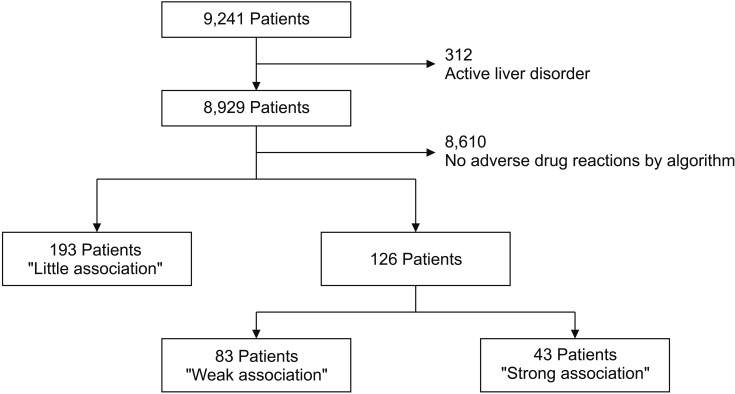
From January 2009 to December 2012, the number of patients who had been prescribed a statin for the first time and had a record of an ALT or ALP level was 9,241. The number of patients who had been diagnosed with active liver disorder within 1 year was 312, and they were excluded from our ADR assessment. Therefore, we applied the ADR assessment algorithm to the final number of 8,929 patients. Table 2 summarizes the patient demographics. The data of 8,929 patients were processed according to the algorithm, and data of 319 patients included some suspicious figures that indicated the possibility of ADRs (3.5%, 319/9,241).
Among these patients, the number of patients who were using concomitant drugs was 193, and we assessed these cases as Litt_AS. Among the 126 patients who were not using concomitant drugs, 0.9% (83/9,241) presented abnormal records of an ALT or ALP level at the baseline. They were classified as Weak_AS because they could have had other causes of abnormal liver function test results. We classified the remaining 43 patients as Str_AS, and they comprised 0.5% (43/9,241) of the total. Finally, the Str_AS and Weak_AS cases comprised 1.4% (126/9,241) of the total (Figure 2).
3. EMR Chart Review
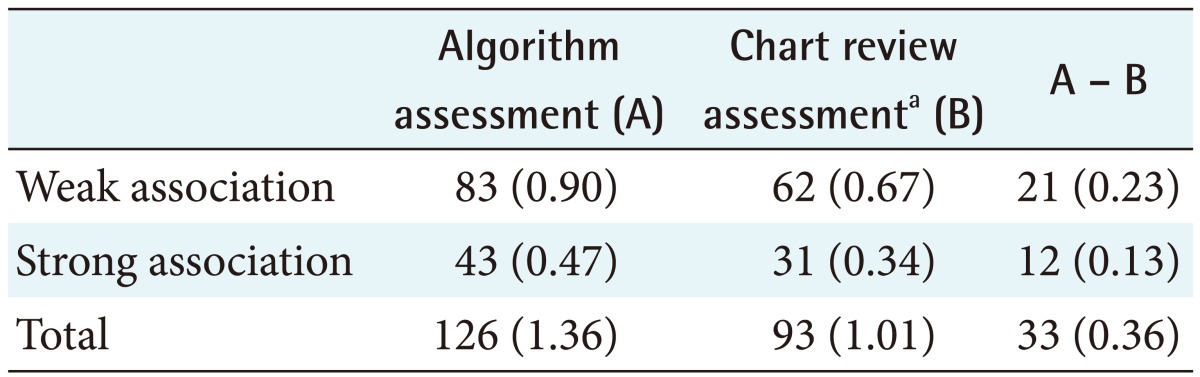
After conducting a chart review of patients classified into Str_AS and Weak_AS cases by the algorithm, we checked the numbers that were assigned to ‘Certain’, ‘Probable’, and ‘Likely’ categories in accordance with WHO-UMC causality groups. Through a chart review of 126 patients who were not likely to have ADRs, 30 patients were determined to have coexisting diseases that increased their ALT or ALP levels. These diseases included fatty liver, alcoholic cirrhosis, and chronic hepatitis B. Moreover, some concomitant drugs were found. These drugs were immunosuppressants associated with hepatotoxicity, such as cyclosporine and azathioprine. These drugs were prescribed to transplant patients.
Thus, the 21 patients who were classified as Weak_AS through the algorithm might actually have been classified as Litt_AS (18 coexisting diseases: fatty liver, alcoholic cirrhosis, chronic hepatitis B; and three cases of concomitant drugs: immunosuppressant cyclosporine, azathioprine). The 12 patients who were classified as Str_AS through the algorithm might have actually been classified as Litt_AS on account of the concomitant drugs. Therefore, the algorithm finally determined that ADR occurred in 93 patients, and the rate of ADR occurrence was 1.0% (Table 3). The performance of the algorithm was verified through PPV that yielded a result of 73.8% (93/126; 95% confidence interval [CI], 69.2%–77.6%).
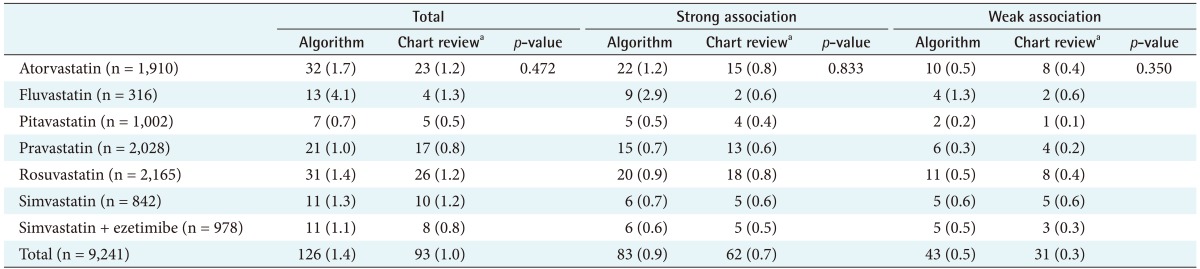
4. Result of Hepatotoxicity Analysis among Statins
We verified the differences between statins in terms of detection of ADR. In the case of fluvastatin, the incidence rate of side effects that affected the liver seemed to be higher than the rates for other statins. However, no difference was observed between statins in Str_AS (p = 0.833) and Weak_AS (p = 0.350) cases (Table 4).
Go to :
IV. Discussion
Statin-induced liver injury increases the AST or ALT level. Its incidence is reported to be 0.5%–2.0% [151617]. Some studies have reported that statin use does not lead to liver damage and that there is no correlation between ALT increase [1518] and statin use. Moreover, it has been reported that any increase in ALT is temporary and reversible [1920]. That is, there is liver damage, but it is not severe, according to recent reports. However, some controversy still exists regarding the effects of statins. Current guidelines demand caution when ALT increases after statin use. In Korea, the guidelines state that when the AST or ALT level in a patient reaches thrice its normal value, statin use needs to stop. For Asian patients, it is understood that even more special caution is recommended while using statins. In Korea, prior to the first-time use of statin, baseline AST or ALT is measured, and after statin use begins, re-checking at 6 weeks and 12 weeks is recommended. In general, statin-induced liver injury is naturally reversed and normalized if the patient discontinues the use of statins. However, in rare cases, idiopathic acute liver failure, which is associated with statin use, causes irreversible liver damage, eventually requiring a liver transplant or causing early death [2122]. Therefore, detecting ADRs at an early stage is necessary to prevent statininduced liver injury from causing serious damage. Because patient safety is of critical importance, detection of an ADR at an early stage is crucial.
EMR data include data for detecting the occurrence of ADRs, such as the time of drug prescription, symptom appearance, and detailed clinical progress. Therefore, EMR data may be a source of information for detecting potential ADRs. In addition, screening specific laboratory findings by using EMR data enables the continuous monitoring of a large number of patients, while using fewer data resources than a chart review [2324]. The Sentinel Project of the US Food and Drug Administration [25] analyzes ADR signals from multi-site EMRs. In addition, the Korean Comparison of the Laboratory Extreme Abnormality Ratio (CLEAR) algorithm analyzes ADR using laboratory findings [26]. However, neither can accurately detect the specific ADR of a particular drug for an individual patient because these studies were developed to detect a number of ADRs for large-scale drugs. Thus, in terms of individual patient safety, both a scientific methodology and proof that an individual specific ADR can be detected via ordinary monitoring using EMRs are needed.
Automatic ADR assessment through the proposed algorithm can detect drug-induced ADR at early stages. As determined by the algorithm, the occurrence rate of liver injury was 1.4%. The PPV-associated accuracy was 73.8%, which was somewhat low. The reasons for this low result were that the diseases coexisting with liver disease were not completely filtered by the algorithm, and not all of the concomitant drugs that cause hepatotoxicity were considered by the algorithm [2728]. This may be because information about a rechallenge of statins specified by the WHO-UMC standard was not included in the algorithm. The current algorithm is very simple and will be enhanced in subsequent work. If the current algorithm is revised to exclude any coexisting liver diseases and include the remaining concomitant drugs, the performance of the algorithm will improve. Moreover, liver injury due to statin use could be assessed with greater speed and accuracy. Meanwhile, the algorithm's rapid automatic ADR assessment can replace manual ADR assessments. The algorithm can assess ADRs with a blood test in a shorter amount of time. During treatment, doctors check important items that cannot be automatically assessed by the system. Thus, the time required to confirm the occurrence of an ADR will effectively decrease.
Our algorithm includes concomitant drug information, diagnosis information, and clinical test information to decrease errors in the ADR assessment. Because we identified improvements for the algorithm through the results of the chart review, the core elements of this algorithm are coexisting diseases, lab test results, and concomitant drugs. It should be noted that the CLEAR algorithm has some limitations because it checks only for abnormalities of laboratory tests to detect ADRs [26]. Furthermore, in the study of Sai et al. [29] of the development of an algorithm to detect statin-induced myopathy, ADRs were assessed by medical practice, adjustments of the times of ADR events, diagnoses, and laboratory data. However, medical practice and adjustments of the times of ADR events are limited by the requirement of frequent blood tests; thus, we could not apply this method to our algorithm based on the results from outpatients visiting every three months. Therefore, we included concomitant drug information, diagnostic information, and laboratory test results. We compared the prescription dates of the concomitant drugs with the occurrence dates of ADRs. To confirm the effects of the concomitant drug on increases in liver enzyme levels, we checked whether the liver enzyme levels were normalized after the patients stopped using the concomitant drugs. Based on this work, our study can be directly applied in real practice and can be useful when upgrading the algorithm later because there are diverse data in EMRs. Beside ALT or ALP, additional necessary laboratory items can be added.
Despite the above contributions, this study had some limitations. When applying the data extracted from EMRs to the developed ADR assessment algorithm, we found that almost 40% of the patients did not have the necessary information. Therefore, the EMR structure should be improved so that related tests can be performed before a drug is prescribed, and the results of the blood tests can be automatically recorded [26]. Furthermore, this research did not access real clinical ADRs that were not discovered by the actual algorithm. In other words, sensitivity and specificity were not identified. However, there was no significant difference between the incidence rate of statin-induced liver injury in many previous studies and the incidence rate of statin-induced liver injury estimated by the algorithm in this study. Moreover, the algorithm was developed without considering that patients may have stopped using statins or changed the type of statin they were using. These aspects will be addressed in subsequent work. Additionally, because coexisting diseases were recorded as free descriptions in the outpatient record, the analysis was not speedy. This information was only found through the chart review. Therefore, these data must be recorded not as text but with corresponding codes in the EMR. Thus, improvements in EMR systems are necessary to enable easy extraction of data [2630]. Many weak points regarding the proof methods of this research exist, but they will be continuously addressed and backed up in future studies; we hope this research will be considered as the first step in this process.
It is desirable to establish a gold standard regarding adverse drug effects by detecting clues of ADR while monitoring side effects and devising countermeasures. However, for drugs of which side effects are already known, if drugs that can prevent these side effects can be preferentially prescribed, continuous monitoring should be systematically possible based on indices of side effects. With such a method, the time required for doctors to prescribe drugs and the length of time during which patients suffer side effects should be minimized. In our study, to detect early statin-induced liver injury, we developed an automatic ADR assessment algorithm that uses the records of coexisting diseases, laboratory tests, and concomitant drugs. Nevertheless, the current system algorithm that we created is too simple. We expect that a more reliable algorithm can be created if we conduct and supplement clinical studies in terms of adverse drug effects. The performance of the algorithm is expected to be improved through larger studies, although the algorithm cannot perfectly detect hepatotoxicity. In addition, we look forward to the clinical application of this algorithm after further validation.
Go to :
 XML Download
XML Download