

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
The term ‘cancer survivor’ was conceptualized in the New England Journal of Medicine of the United States and includes the categories of acute, expanded, and permanent survival according to cancer survival phases [1]. Specifically, the divisions became ‘acute survival under treatment following cancer diagnosis, expanded survival under follow-up observation following aggressive fundamental treatment or disease remission’, and ‘permanent survival with complete recovery or absence of cancer progress based on little likelihood of recurrence’. This scalehas since developed into an evidence-based concept of cancer survival and has become the cornerstone of a new approach to survivors.
Completion of cancer treatment is highly meaningful for cancer patients. Those who have completed cancer treatment, or patients whose cancer treatment has been completed, are often called cancer survivors. Initially, this term referred to those who had survived without recurrence for 5 years after diagnosis with or treatment for cancer. Two of the most important factors of health management for cancer survivors are primary cancer treatment and recurrence follow-up. However, most cancer survivors fail to receive evidence-based service because they approach service based on personal experiences after completion of treatment.
Cancer statistics are focused on the survival of incidence, mortality and prevalence. Cancer survivors have been classified by the ‘survival period’; however, such classification is not appropriate as a healthcare service model to reflect the diverse needs of long-term cancer survivors. About 1,370,000 people in the Korea had a cancer diagnosis by the end of 2013 [2]; some were diagnosed the previous week, whereas others were diagnosed more than 10 years previously. With 225,000 new cases of cancer diagnosed in 2013, the number of people living with cancer is rising every day [3]. If current trends continue, there will be 3 million cancer survivors (living people who have had a cancer diagnosis at some point in their lives) by 2030 [4]. Only 20 years ago in Korea, 6 out of 10 patients with cancer did not survive for more than 5 years after their diagnosis. The “10-Year Plan for Cancer Control” that started off in 1996 contributed to raising the cancer survivability rate to 70%. However, as national cancer policy was mainly focused on battles against cancer, the problems faced by cancer survivors were neglected. Because of this situation, cancer survivors have been fighting second battles with depression, aftereffects, social isolation, and other agony [5].
The National Cancer Survivorship Initiative (NCSI, established in 2007), with the aim of establishing and improving the evidence base on survivorship, implemented a project of classifying cancer survivors registered in the Cancer Registry. This project aimed to give positive care to people who spent a lot of time in the hospital over several years due to a prolonged survival period and who were vulnerable to distress as a result of cancer treatment. In particular, it aimed to lay the groundwork for post-care for cancer survivors, a new pathway of care [6]. With reference to NCSI's methodology for the new pathway of care, this study aims to establish an evidence base on survivorship.
The purpose of this study is to present a classification model based on ‘care pathway according to needs-based segments.’ It aims to present a good healthcare service model for each treatment period (survival period) in follow-up management for cancer survivor healthcare providers.
II. Methods
1. Survivorship Classification Based on Cancer Care Pathway
The survivors are classified by the ‘survival period’ into four groups: survival for <1 year, for 1 to <3 years, for 3 to <5 years, and for ≥5 years [78]. The annual report of cancer statistics by the Korean Central Cancer Registry (KCCR) presents information on survivors by cancer type according to this classification method. However, there is no healthcare service model for each treatment period in long-term follow-up and treatment for cancer survivors at each of the risky stages that involve recurrence, metastasis, and secondary cancer development. From the pre-treatment to the post-treatment stages, cancer survivors need information about the contents of treatment and the effects of the disease. To improve the quality of patients' lives for their remaining days, it is also necessary to develop a program for positive and constant management.
We refer to the cancer survivor classification of NCSI in the United Kingdom [6]; to render classification into five stages of ‘Diagnosis and treatment,’ ‘Supportive care,’ ‘Monitoring,’ ‘Progress illness,’ and ‘Hospice care,’ the concept of primary ‘care pathway’ for cancer management was regarded as the period from the diagnosis of cancer to a point before the pre-death stage of terminal cancer.
2. Care Pathway for Breast Cancer Survivors
1) Diagnosis and treatment
According to the latest annual report of cancer statistics by KCCR, 225,343 cancer patients (113,744 males and 111,599 females) were newly registered in 2013, which represents a drop of 0.39% from 2012 [7]. The ‘Diagnosis and treatment’ suggested target those under cancer treatment, which involves surgery, anticancer therapy, gene therapy, radiotherapy, and immunotherapy.
This stage is one in which cancer treatment following diagnosis is required; it targets those developing cancer in the year concerned. The difference between incidence and this stage is as follows. The idea of ‘incidence’ is the number of new cases per population at risk in a given time period [9]. The ‘Diagnosis and treatment’ stage is included up to the period of treatment (for example, a period of less than one year after the initial diagnosis of cancer). For the year 2010, this stage involves those who developed cancer in 2010. Those developing cancer in the year concerned.
2) Supportive care
‘Supportive care’ for cancer survivors refers to a post-treatment stage after the completion of surgery and anticancer therapy and targets those for whom physical activity can be tested for rehabilitation services; this stage involves recovery from fatigue, physical competence recovery, and aerobic exercise.
In this stage, survivors for the first year following cancer diagnosis need support and rehabilitative treatment and are supported with physiotherapy, occupational therapy, dietetics, life cycle assessment, and planning after cancer treatment. For estimation purposes, the number of one-year survivors is drawn from the number of those developing cancer in the previous year and the total number of cancer patients; Those developing cancer in the previous year × (1 + one-year survivors/100).
3) Monitoring
‘Monitoring’ targets cancer patients who have survived for >2 years after diagnosis with cancer. Those with progressive diseases, such as recurrence and metastasis, are excluded from monitoring.
In this stage, those surviving for 1–5 years and for >5 years after the initial cancer diagnosis are monitored so that they can lead healthy lives. For estimation, the number of those with progressive diseases in the year concerned is excluded from that of patients surviving for >1 year; Number of patients surviving for 1–5 years – Number of those with progressive diseases.
4) Progress illness
‘Progress illness’ was defined as high risk of death due to recurrence of the original cancer in a neighboring region, metastasis to another region, or development of a new type of cancer unrelated to the original cancer following cancer treatment. Most of the patients dying within 2 years after diagnosis reportedly died of metastatic cancer [10].
Since most of the patients who died within 2 years of their diagnosis died of metastatic diseases, this stage is to determine diseases currently in progress. Since dates for abnormal scans are not collected on a regular basis, the average survival period was considered by using the number of deaths in the year concerned for estimation; Number of deaths in the year concerned × (average survival period − 1).
5) Hospice care
‘Hospice care’ is part of an effort to recover human respect and refers to services that involve comprehensive care for terminal cancer patients with a short time to live and their families in physical, psycho-social, and spiritual aspects.
This stage involves managing patients who require palliative care. The number of deaths in the year concerned is used for estimation. However, those dying in the year of cancer diagnosis can be included in the two stages of diagnosis and treatment and palliative care. So the number of those dying in the year of cancer diagnosis was excluded from the number of those developing cancer in the year concerned; Number of deaths or number of those developing cancer in the year concerned × [1 − (1 + one-year survivors / 100)].
3. Data Source
Within the scope of privacy protection, a sample cohort database (DB) of the National Health Insurance Service (NHIS) was established on the basis of the national health information DB to disclose data for research. The sample cohort DB was built in connection with qualification data, details on medical treatment, and medical check-up data, which contained socio-economic variables (place of residence, date of death, cause of death, income level, etc.) for 9 years from 2002 to 2010 in a sample of approximately 1 million persons or 2% of the whole nation (50 million persons).
The sample cohort DB was built to estimate the number of cancer survivors through the following stages: In the first stage, only patients with the principal condition of ‘C50x’ were drawn from the ‘specification data’ of the ‘patient clinical DB.’ In the second stage, the whole ‘patient clinical DB’ was merged into claim serial numbers to complete to ‘patient clinical DB’ with the principal condition of ‘C50x.’ In the third stage, ‘qualification and examination DBs’ were merged into personal serial numbers to complete ‘qualification’ and ‘examination DBs’ for individuals. In the fourth stage, ‘patient clinical DB’ with ‘C50x’ and ‘qualification’ and ‘examination DBs’ for each ID were merged into personal serial numbers to determine the yearly transition for breast cancer patients (Figure 1).
III. Results
1. Estimation Results for Breast Cancer through Care Pathway
1) Cancer statistics data of KCCR
We analyzed the cancer statistics data of KCCR collected from 2008 to 2012, in order to establish a service provision model. The survivor group after diagnosed with breast cancer was classified into (1) patients under active treatment with surgery and chemotherapy; (2) survivors with relatively fewer side effects and no sign of a recurrence; and (3) cancer survivors under palliative treatment after a recurrence.
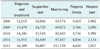
The survivor group was categorized into five stages, including ‘Diagnosis and treatment,’ ‘Supportive care,’ ‘Monitoring,’ ‘Progress illness,’ and ‘Hospice care,’ using these categories, the scale of breast cancer survivors was estimated. The result of estimation of results of the estimation of the number of breast cancer survivors according to care pathway by survival stage is shown below. There were 16,600 cases of the incidence of cancer in 2012 in the ‘Diagnosis and treatment.’ Among the cases of the incidence of cancer in the previous year, the number of one-year survivors was 18,000; these were included in the ‘Supportive care.’ In the ‘Monitoring,’ 111,700 survivors maintaining healthy lives were included. Total 4,000 survivors were checked to identify an ongoing disease and included in the ‘Progress illness.’ In the ‘Hospice care,’ 2,000 end-stage cancer patients requiring hospice care were included (Table 1).
2) Sample cohort DB of NHIS
The number of breast cancer survivors was estimated on the basis of the NHIS sample cohort DB between 2004 and 2010. According to the NHIS cohort DB, which covers 9 years, there were approximately 1,063,645 cancer patients and the number of cancer patients was gradually increasing. Most OECD (Organization for Economic Cooperation and Development) member countries showed high occurrence rates of breast and colorectal cancers; South Korea also saw a breast cancer occurrence increased due to the increase in obesity and a westernized dietary life. The number of 5-year patients was estimated at approximately 1,073 in 2004; the number of 5-year breast cancer patients was estimated to be approximately 2,593 in 2010.
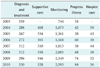
In comparison with the data of National Cancer Registration and Statistics (NCRS) of Korea, as reported on an annual basis, the incidence of breast cancer patients increased from 12,612 in 2008 to 14,345 in 2010. In the sample cohort DB, the number increased from 312 in 2008 to 330 in 2010. During the breast cancer survival period between 2003 and 2010, the number of those surviving for 1–5 years increased dramatically from 744 in 2003 to 2,593 in 2010 (Table 2).
Based on the sample cohort DB of the National Health Insurance Service (NHIS), breast cancer treatment recipients from 2004 to 2010 were analyzed according to the classification model this research suggests (The year 2002 was excluded from the analysis. For the year 2003, the values of ‘Supportive care’ and ‘Hospice care’ were not estimated, so this year was excluded from the analysis).
First, diagnosis recipients increased in number from 288 in 2004 to 330 in 2010; however, the occurrence rate decreased from 15.4% to 9.8%. Second, supportive recipients decreased in number from 408 in 2004 to 328 in 2010, and the occurrence rate of rehabilitation recipients decreased as well from 21.9% to 9.7%. Third, monitoring recipients increased in number from 1,073 in 2004 to 2,593 in 2010; the occurrence rate of post-care recipients also greatly increased from 57.4% to 76.9%. Fourth, progress recipients did not change much in rates, from 2.2% in 2004 to 2.5% in 2010. Fifth, hospice recipients decreased constantly from 3.2% in 2004 to 1.1% in 2010 (Figure 2).
2. Age-Specific Survival Rates
‘Diagnosis and treatment’ (2009) was performed for 6 subjects (2.03%) aged 30–34 years, for 58 subjects (19.59%) aged 50–54 years, and for 29 subjects (9.80%) aged 60–64 years (Figure 3A); ‘Monitoring’ (2009) was performed for 30 subjects (2.10%) aged 30–34 years, for 326 subjects (22.78%) aged 50–54 years, and for 160 subjects (11.18%) aged 60–64 years (Figure 3B). Breast cancer was most commonly diagnosed among women aged 35 and 64 years [3]. Breast cancer showed inverted U-shaped survival rates by age.
IV. Discussion
The goal and vision of follow-up management for providers to survivors through ‘cancer survivor classification based on care pathways’ are as follows:
First, it is necessary to help survivors restore their daily life routines following cancer treatment (for target). Treatment of primary cancer and recurrence follow-up are two of the most important factors of health management for cancer survivors. Every patient enters a treatment system following cancer diagnosis. From the beginning, while some of these patients cannot obtain any other treatment than palliative care, most of them get treatment for the purpose of complete recovery. While the term ‘cancer survivors’ in the current meaning refers to cancer patients in all stages from diagnosis through the pre-stage of terminal treatment, as well as their families services need to target patients in a shorter period before recurrence or secondary cancer occurrence following the completion of initial treatment. The specific reasons for this are as follows: patients for whom treatment has been completed need to be included in the category of survivors and different types of care apply to initial treatment, the period before recurrence following the completion of the initial treatment or secondary cancer occurrence, and terminal cancer treatment. Therefore, it is difficult to identify problems when, taking all these periods into account. So, the system can be restricted to a certain period for follow-up management after the completion of the initial treatment; this will make it is easy to implement and can lead to high recognition in general when a cooperative healthcare delivery system between healthcare consumers and primary care for cancer survivors is introduced.
Most cancer patients may complete treatment a year after cancer diagnosis and manage the disease by themselves without special types of treatment other than regular visits to the hospital for further management. They need long-term management because they may not only become more uncertain about their disease but also because they can become anxious about metastasis [11], become afraid of recurrence, and have conflicts concerning their survival [12]. In particular, since 92.0% of breast cancer patients may reportedly see it recur postoperatively within 5 years [13], it is very important to inculcate constant ‘health-promoting behavior’ to prevent recurrence. Health-promoting behavior is an essential factor to prevent the recurrence of cancer and maintain and promote the health of cancer patients [14]. However, most cancer patients tend to believe that they do not need any more healthcare services when their treatment is completed [15]. Harding [16] suggested that breast cancer survivors participating in health-promoting behavior can control their own health status, have fewer chances of recurrence, see physical health promoted, and relieve psychological stress, such as anxiety, depression, and concern.
Evidence suggests that by reducing chances of recurrence and improving their overall physical health, survivors who engage in health-promotion behaviors experience improved quality of life by achieving some control over their own health; that control may contribute to moderating their level of psychological distress, including lowering their levels of anxiety, depression, and worry. Therefore, health-promoting behavior for breast cancer survivors can be an important factor to reduce the chances of recurrence.
Second, it is necessary to develop a cooperative healthcare delivery system model (for healthcare institutions and the medical staff) applicable to each survival period (for providers).
Cancer survivors can spend significant amounts of time in hospital many years after diagnosis. With increasing survival, it is likely that more people will suffer from the consequences of their cancer treatment in later years. The current focus of cancer care is on initial diagnosis and treatment and the last year of life [8]. According to the big data analysis of NHIS, post-care is badly needed for the monitoring of recipients, namely survivor, who that have been increasing rapidly in numbers [17]. According to “development research on unified service system for cancer survivors centered on a regional cancer centers,” appointed hospitals have met with many difficulties and have responded that “Time and financial resources are insufficient to build cooperative systems” (77.3%) and that “There exist no official systematized communicative channels for mutual cooperation” (61.4%) [4]. As such is the case, “cancer patient self-implementation rates” (rates of patients with cancer utilizing regional medical institutions) are only at 27.5% in Gyeongbuk, 35.2% in Choongnam, and 48.1% in Gyeongnam. It is concluded that systems to meet the situations and requests of cancer survivors must be developed.
The United Kingdom implements a service delivery model based on care pathways for each type of cancer. In particular, the country has created standardized guidelines regarding who should provide treatment summaries for cancer survivors in each stage to patients and how (http://www.ncsi.org.uk/). To implement an intervention program, the North Trent Cancer Network divided colorectal cancer survivors into a total of eight stages according to the survival period and complication status [6]. This was the second attempt to use readily available data to segment the population living with cancer into needs-based phases and allow targeting of interventions and redistribution of resources. These data convey the critical need for the development of survivorship services and shows the survivorship population into needs-based phases, which will allow targeting of interventions and redistribution of resources [10]. The limitations of this study are mentioned in the NCSI [10], the nature of a ‘Progress illness’ makes it difficult to estimate the number of people who have progressive cancer, but who are not in their last years of life, and as such will have particular health needs.
In this study, a prototype of an intervention program, implemented according to the survival period and complication status for breast cancer patients, is expected to be drawn on the basis of a cancer survivor classification plan based on care pathways. The study also aims to design a post-treatment management program for those getting short-term radiotherapy, which has relatively fewer side-effects, following surgery and anticancer chemotherapy and anticancer hormone therapy over several years; the study also targets follow-up management for the group of survivors who have no sign of recurrence after completion of all these adjuvant types of treatment.



 XML Download
XML Download