

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Electronic Medical Record (EMR) systems have numerous benefits, such as improvement in the quality of care, medical error prevention, and reduction of unnecessary care costs. However, one major barrier to the adoption of EMR systems is the cost issue [1-11]. As a result of searching on PubMed, 5 papers related to the economic evaluation of the EMR were identified (Table 1). Wang et al. [5] performed a cost-benefit analysis (CBA) of EMR with a computerized physician order entry system (CPOE). The result was a positive return on investment (ROI), and the benefits were mainly from savings in drug expenditures, radiology tests, billing errors, etc. Barlow et al. [7] assessed the effects of EMR assuming 5 years based on 1 year experience. The maintenance of paper-charts decreased and the reimbursement process was improved. Hillestad et al. [6] reported more than $81 billion in savings annually after the adoption of EMR. The potential savings and costs were based on a broad literature survey. Kaushal et al. [8] analyzed the effects of CPOE systems based on published studies, interviews with experts, and internal documents. The major cumulative savings were from renal dosing guidance, nursing time utilization, specific drug guidance, and adverse drug event prevention. Himmelstein et al. [4] reported no reduction of overall costs in hospital computing after an annual survey of computerization in about 4,000 hospitals from 2003 to 2007.
They demonstrated that the EMR could result in a positive financial ROI [5-8]. However, such financial benefits were reported to be still premature at best, and it would be difficult to realize direct economic benefits, as Himmelstein et al. [4] asserted [8-10].
These conflicting results likely came from hypothetical estimation based on secondary data, such as the Medicare Cost Report, the Medical Expenditure Panel Survey, and other broad surveys [4-8]. Therefore, there are some limitations to reflect economic benefits in real-life clinical practice. Therefore, there is a real need for further analysis to determine whether EMR is financially cost-effective in real-life clinical settings.
II. Methods
This study analyzed the economic effects of an EMR system using a CBA, based on differential costs of managerial accounting. In this paper, we excluded any qualitative factors, such as improvements to patient safety. These factors are much more important issues in healthcare service, but are not easily converted into monetary values. This study focused on using tangible items which can be measured in managerial accounting. In conclusion, this study discussed cost shifting after EMR adoption at a tertiary hospital and its implications.
1. Study Site
Samsung Medical Center (SMC), founded on November 9th, 1994, is an academic nonprofit tertiary hospital, with 2,000 beds and about 6,500 staff, including over 1,300 doctors and 2,000 nurses. In 2013, more than 8,500 outpatients visited SMC per day.
This study defines the EMR system as a system that allows physicians to generate patient records during outpatient encounters and to maintain them. Implementation of the EMR system for inpatient care started in 2001 and was completed in 2003. Paper-charts were completely removed from the wards during this process. The SMC began the development of an EMR system for outpatients in January 2006. Hospital-wide adoption was completed at the end of 2008 [11] (Figure 1). Even though the EMR system for inpatients is interfaced to EMR system for outpatients, the costs for developing the system and the benefits were completely independent; paper-charts were separately managed at the time of implementation, and the systems were too dissimilar. Thus, this study only considered costs and benefits of the EMR system for outpatients.
2. Cost-Benefit Analysis
In this study a CBA based on cash flows of SMC was carried out. The detailed items of costs and benefits were determined based on differential costing, which is mainly used for decision making in managerial accounting, after comparison of workflows between the paper-chart system and the EMR system [12] (Table 2). This was a conservative CBA in that this study excluded any potential or qualitative benefits [2,3,8,10]. The financial costs and benefits were obtained primarily through the SMC accounting records. The costs of EMR implementation were the actual measured value. However, the benefits were calculated by using the difference between actual measured values and expected values without the EMR system. Therefore, when data were not available, capital amounts were determined by the opinions of experts, such as medical record administrators, care floor nurses, and IT engineers. The measured amounts were converted to present values (PV) using SMC's expected interest rate. Then, the net present value (NPV), the benefit-cost ratio (BCR), and the discounted payback period (DPP) were calculated.
The period was set to 8 years, 2006 to 2013, rather than the 5- or 10-year periods considered in previous studies [4,5,7]. The 8 years were divided into 2 subgroups: the first 3 years for the partial implementation of EMR and the second 5 years during which the EMR system was fully operational.
1) Costs
The newly implemented EMR system created additional costs that were not incurred with the paper-chart system. There are 2 cost categories: the system costs and the induced costs [5,10,13]. The system costs include the direct costs to build the system infrastructure, to develop the EMR applications, and to purchase office supplies [5,13]. The induced costs were required to smooth the EMR adoption. The first cost was to scan the existing paper-charts into the EMR system. The second cost was to provide assistance to doctors through medical transcriptionists (MTs). MTs are typists who enter medical records into the EMR system instead of the physicians at the point of care.
2) Benefits
The benefits include cost reductions and additional revenues. The cost reductions originated from cost savings due to elimination of the paper-chart system. There were 5 types of cost reductions: 1) the reduction of supplies for paper-charts, 2) the disposal of storage facilities, 3) the reduction of full-time equivalent (FTE) employees for paper-chart management, 4) laying off of clerks from the outpatient clinic setting, and 5) the reduction of supplies for medical devices [5-7,11]. These cost reductions fundamentally come from elimination of the paper-chart system operation costs. These operation costs were reduced or eliminated after adoption of the EMR system. This study estimated the reduced amounts based on SMC's accounting practices of 2006. The cost reductions were influenced by the number of daily outpatients, yearly new outpatients and interfaced medical devices. To ensure greater financial accuracy, the benefit was adjusted using the consumer price index (CPI), rental expense, and personnel expenses.
Additional revenues were generated from both remodeling of paper-chart storage rooms and the MTs' contribution. This study analyzed the number of outpatients examined in the remodeled clinic rooms. The incremental revenues were calculated by multiplying those numbers with both the yearly revenue per room and the contribution of the space to revenue. To calculate benefits of the MT support, we compared the average number of outpatients per examination session before and after EMR adoption. The differences were used to assess the additional revenue due to the MT support.
3) Present value and discount rate
All costs and benefits were converted to 2006, US currency (US$). The SMC's expected interest rate was calculated by adding the certificate of deposit (CD) rate to 1.7%. The CD class is non-guaranteed corporate, the time to maturity is 3 months, and the credit rating is A+ [14,15]. If the CD rate is 3.5%, the interest rate will be 5.2%. The starting point for analysis was set from 2006, when the SMC started the development of the EMR system. The PV is a financial amount discounted by the yearly interest rate on an accrued basis.
4) Outcomes of analysis
The primary outcome is the cumulative NPV which subtracts the PV of cost from the PV of benefit for the eight-year period. The second outcome is the BCR, which is the PV of the benefit divided by the PV of the cost. The third outcome is the DPP, meaning the time to reach the breakeven point.
5) Case analysis
The SMC's expected payback period is 5-year. The SMC invested in a paper-chart scanning system to scan existing paper-charts to improve user convenience. It also provided MT assistance to alleviate the doctors' resistance to change. The combination of these conditions could facilitate another 3 case analyses.
III. Results
This study scrutinized the factors affecting both costs and benefits in order to calculate their financial value. These factors include outpatient numbers, rental fees, personnel expenses, CPI, CD rate, and the revenue per patient. Data from 2006 to 2012 were mainly obtained from SMC's accounting records, whereas data for 2013 were based on the SMC's management planning. The results are summarized in Table 3.
1. Costs
As described in the Methods section, costs were divided into 2 categories; the system costs and the induced costs. Among the system costs, the purchase cost of the system infrastructure in 2006 was US$1,241 thousand with a 5-year warranty included. Maintanence costs have been incurred since 2010. The development costs of the EMR viewer and the medical device interface system (MDIS) were US$1,006 thousand in 2006, US$1,274 thousand in 2007, and US$315 thousand in 2008. Maintanence costs for these applications have been incurred since 2009, and increased by 5.5% every year under Korean government guidelines. Office supplies, such as PCs, monitors, printers, etc., were purchased and the financial costs were US$306 thousand in 2006 and US$286 thousand in 2007. Maintaning these items costs 10% of the initial investment after the 1-year free warranty. Among the induced costs, the cost of investing in the existing paper-chart scanning system was US$724 thousand in 2008 and US$519 thousand in 2009. The personnel costs for MT support also have been incurred since September 2006. The cost for MT support was US$166 thousand in 2006. The PV of all accrued costs was US$16,054 thousand.
2. Benefits
To assess the benefits of cost reduction, we measured the supply consumption of September 2008 and compared it to the equivalent figures for 2006 and 2007. The supplies included paper-chart holders, labels, A4-size paper, gloves, etc., which were used to build and maintain the paper-charts. As a result, about 1.3 million pieces of A4-size paper were saved in 2008. The transportation cost of the paper-charts to the outside storage facilities and the building costs related to the automated cabinets and carousel facility were also saved. The PV of the supply savings was US$1,076 thousand.
Scanning existing paper-charts helped to eliminate 495 m2 of indoor storage and 627 m2 of outside warehouse space. According to our analysis, about 1 m2 was needed to store the paper-charts of about 910 new outpatients, and an additional 150 m2 per year were needed. Thus, the rental fees for the storage space were converted into a financial benefit. The PV saved from storage was US$703 thousand.
The paper-chart management FTEs built, delivered, and collected the paper-charts. After adoption of the EMR system, the number of the FTEs was greatly decreased from 28 in 2007 to 1 in 2009, whereas the number of outpatients per day significantly increased. The actual decrease in 2009 was 27. However, this study applied 32 FTEs since this study had to consider the growth of outpatients, which would have affected the number of the paper-charts to be delivered. The figure for the 32 FTEs was not recorded in the accounting records, but it was a conservative estimate from the chief of the department of medical records, who had vast experience in administration of the paper-charts. She expressed that the number depended only on the linear relationship to the growth of outpatients, but it did not consider the expansion of the buildings and the distance between them. There were only 7 actual reduced FTEs in 2008, but it was estimated that up to 36 FTEs would have been reduced in 2013. The only job left is to scan the signed consent forms into the EMR system. The PV of the FTE reduction was US$4,231 thousand.
Registered nurses in charge of the outpatient care floors showed that there were also 11 clerks fully dedicated to the management of the paper-charts, and they were laid off after the EMR adoption. It was very difficult to calculate the number of clerks on the outpatient care floors because the management of paper-charts on the floor was usually shared by all of the clerks. The registered nurses expressed that there were about 20 separate outpatient care areas, but only 11 clerks were moved to another department or did not have their contracts renewed. It is also conservative in that it did not consider the expansion of a building with about 10 outpatient care floors. The PV from the decreased clerk FTEs was US$990 thousand.
In 2009, the number of medical devices interfaced with the EMR system through the MDIS was 352. The MDIS has saved supplies for medical devices such as A4-size paper, photographic paper, and roll-paper. The reduced cost for only 126 devices in 2006 was US$7 thousand. The yearly cost reductions were proportional to the number of interfaced devices. The PV of the savings was US$944 thousand.
Among the benefits, additional revenues have been recognized from the paper-chart storage areas. The indoor storage was remodeled into clinic rooms for outpatient examinations. The revenue from this clinic was US$17 thousand in 2009, considering the contribution (4.15%) of the remodeled space to the revenue. The PV of the generated revenue was US$125 thousand.
After adoption of the EMR system, 5 paper-chart temporary storage rooms on the outpatient care floors were also converted to clinic rooms. In this case, the contribution of the remodeled space to revenue was 4.02%. The PV from the clinic rooms was US$1,646 thousand.
This study also found that the MT assistance also contributed to the growth of the number of outpatients per examination session. The contribution degree is counted as 25% of the growth; about 1.2 outpatients per the session they attended. The PV of additional revenue from the MT contribution was US$9,956 thousand. The total PV of all accrued benefits was US$19,672 thousand.
During the analysis period, the cumulative NPV and the BCR were US$3,617 thousand and 1.23, respectively. The DPP was about 6.18 years (Table 3).
Total personnel costs for MT support were US$8,612 thousandwhich was 53.6% of total accrued costs (US$16,054 thousand). The direct costs for the EMR applications and the system infrastructure were 21.9% and 10.0%, respectively. These 3 items covered 85.5% of the total costs.
Among benefits, additional revenue from MT support was also the largest at 50.6% of the total accrued benefits (US$19,672 thousand). The reduction of chart management FTEs contributed 21.5% to the benefits. The additional revenues incurred from remodeling of paper-chart storage areas accounted for 9.0% of the benefits. These 3 items also covered 80.5% of the total benefits.
Both the costs and the benefits are largely influenced by the MT support, which was introduced to smooth EMR adoption. Scaning the existing paper-charts and storing them in the EMR system allowed the remodeling of the storage rooms into outpatient examination rooms. The benefits from this remodeling were also a large proportion of the total benefits. Looking at these results, the combination of the MT support and scanning the existing paper-charts could lead to different results. Therefore, this study attempted a case analysis with these 2 items.
3. Case Analysis
The SMC invested in both scanning the existing paper-charts and MT support with the EMR adoption. In other cases, one of these might be excluded or both might be excluded. Thus, 3 additional cases were used for the economic evaluation (Table 4).
If a 5-year analysis period would have been applied, the cumulative NPV would have been under 0. However, the cumulative NPV based on an 8-year analysis is greater than 0. Thus, the EMR system can be financially cost-effective, but only if it is used for at least 4 or 5 years after full implementation.
The most cost-effective choice would have been investing in a simple transition from the paper-charts to the EMR system. Without scanning the existing paper-charts and the MT assistance, the cost would have been much lower. The DPP in this simple transition would have been 5.45 years which is a little shorter than in other scenarios. Even though it would be the best choice among other scenarios, it still does not meet the SMC's expected ROI period.
IV. Discussion
It is a very meaningful economic evaluation in that this study performed a formal CBA using actual cash flows of tangible costs and benefits based on differential costs, which is useful for decision making in managerial accounting, in contrast to previous studies that have been based on potential factors.
As the previous studies mentioned, the biggest barriers to EMR adoption in hospitals are capital investment and high maintenance costs. Unfortunately, this study also revealed the same problem [7-11]. However, there is some comfort in that an analysis based on an 8-year study showed EMR to be financially cost-effective, because the cumulative NPV was greater than 0. Analysis covering a 5-year period after full deployment of the EMR system showed positive cash flow. Compared to other industries, it takes much longer to deploy IT systems in the health care industry. The health care industry also tends to use systems for longer periods of time, usually more than 5 years. The SMC, like other hospitals, still continues to use the EMR system actively, even though the SMC has now been using the EMR system for just over 5 years after full implementation. At that point, the EMR in the SMC became financially cost-effective. It is also true that there are various hard-to-quantify benefits that the EMR system contributes. If future research discovers more detailed benefits, such as the elimination of additional FTEs, the economic justification for the EMR system will be more supported.
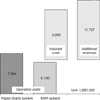
One interesting finding is that the overall costs were increased as the IT paradox, since the induced costs were included for a smooth EMR adoption [16]. However, with careful consideration, it was found that the costs for a simple transition from paper-charts to the EMR system decreased (Figure 2). Although induced costs were incurred, the cumulative NPV was positive as they contributed to additional revenues.
Another interesting finding is that the paper-charts management system was cost-centric (Figure 3). Year by year, the maintenance costs for the paper-charts were growing. However, the EMR system created new revenues according to this study based on differential costs. Thus, the adoption of an EMR system is not a matter of choice, but a necessity for management.
As described in the Methods section, the data for 2013 were based on the SMC's management planning. According to the plan, the estimated number of outpatients per day is 8,368. The actual measured number during the 1st quarter was 8,806. The difference was 438 patients per day, or 5.2% more than planned. This will positively affect the benefits, which are based on the number of outpatients per day. However, there is uncertainty as to whether this positive trend will last for the rest of the year. Thus, this study decided to apply the planned number of outpatients in the analysis.
This is a considerably conservative CBA in that this study did not included any potential benefits, such as the reduction of adverse drug events, as stated by Kaushal and Bates [17]. The benefits are much too great to be ignored. There are many difficulties in measuring values. Sometimes, the accuracy of measurement may generate controversy [4,5,7,10]. It is a limitation that this study does not include such meaningful benefits.
In case of the SMC, the transition time from paper-charts to the EMR took longer than necessary. This helped to relieve inconveniences to users and resistance to change from the doctors. It is really arbitrary to set an analysis period in this type of study. Since different results may be found if the analysis period is varied, the results must be interpreted with careful consideration.
Overall, our findings may not always be applicable in all clinical settings since our study was conducted in a single large academic hospital with a rich digital-based infrastructure. In the case of the SMC, all medical devices have been interfaced with the EMR system. All the existing paper-charts were also scanned into the EMR system. To meet user requirements or management strategies requires higher costs. However, it is difficult to say that the EMR system could not be adopted without such convenient services. Therefore, the results may vary with the hospital size, patient volume, and specific IT investment policies.
Although the adoption of an EMR system at a tertiary hospital resulted in overall growth in administrative costs as predicted by Himmelstein et al. [4], EMR adoption was financially cost-effective since the cumulative NPV was positive. The positive NPV, as Wang et al. [5] suggested, was attributed to both cost reduction and additional revenues. EMR adoption is not so attractive to management in that the DPP was longer than 5 years at 6.18, and the BCR is near to 1 at 1.23. However, the EMR is a worthwhile investment, seeing that this study did not included any qualitative effects, and the paper-chart system was cost-centric.
This study was a considerably conservative CBA in that any potential benefits were not considered. To support the economic justification of the EMR, more detailed benefits, such as the elimination of labor hours, which are not recorded on the accounting record, should be examined. Therefore, we recommend that more cases of tangible benefits of EMR should be reported to accelerate its adoption in the future.






 XML Download
XML Download