

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
In today's era of unlimited competition in all spheres of life, modern people are becoming vulnerable to various types of diseases. Hair loss has begun to attract increasing attention in contemporary society, where outward appearance is very important. Recent trends show that patients exposed to various factors excluding genetic factors and natural ageing, such as environmental pollution, stress from tough competition, and unhealthy eating habits and diet, are escalating. This further becomes a vicious cycle when hair loss itself plays a role in causing alopecia. Anderson [1] emphasized stress as the cause of alopecia and its relapse. Maffei et al. [2] and Fossati et al. [3] showed that hair loss patients have a high rate of morbid personality disorder before diagnosis of alopecia. Although hair loss is a disease that affects daily life, medical doctors argue that it greatly impacts personal life [4]. The constant mental and emotional stress leads to secondary morbidity [5]. Thus, stress due to hair loss is often compared to that due to severe chronic illness or life-threatening disease [6]. Alopecia patients believe that the disadvantage due to a negative image formed by hair loss in the social sphere, including job and marriage prospects and various social activities, tend to cause lack of confidence and self-deprecation accompanied by psychological anxiety, depression, and emotional disorders [7]. Therefore, hair loss should be regarded as an aspect of life requiring more attention than a simple dermatological disease does [4]. Schlenker and Leary [8], define interpersonal anxiety in social situations as anxiety when personal evaluation is expected or its result exists in the real or imaginary order. Leary et al. [9] stated that people often complained of fear of negative evaluation by others and it leads to various secondary diseases. Recent medical research reported the construction of severity adjust model [10], development of hypertension predictive model [11] and development of a tailored follow up management model on hypertension [12] et cetera by using the data mining technique and identifying hepatocellular carcinoma (HCC) by proteomic profiling study of HCC patients through two-dimensional gel electrophoresis (2-DE) and revealed potential candidate cancer biomarkers by artificial neural networks and decision tree (CART) [13] and prognosis of prostate cancer by using artificial neural networks and receiver operating characteristic (ROC) analysis [14]. In addition the data mining technique has been used for treatment of female pattern hair loss with oral antiandrogens [15], the epidemiological analysis of androgenetic alopecia [16] and environmental stress in children or adolescents with alopecia areata [17] et cetera. However, there isn't enough research for the secondary symptoms of alopecia. The present study aims to collect empirical and theoretical data by analyzing the correlation between hair loss and symptoms based on chief complaints of patients with hair loss through the data mining technique. We examined the usefulness of highly reliable data on the identification of patients' symptoms before and after hair loss treatment and prevention of secondary diseases as well as clinical information of patients in the course of hair restoration treatment.
II. Methods
1. Data Collection
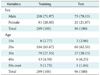
This study was based on patients who visited the Seven Rhema clinic specializing hair loss treatment, which has 2 clinics located at Gangnam and Gangbuk in Seoul, from January 2009 to June 2011. We randomly selected 300 patients, a number we considered sufficient as an n value to construct a model. We selected the data and another 100 patients randomly to develop a model for validation and combined it with constructed models from 300 patients and both used the same items. We analyzed the data from the results of 289 medical examinations; the remaining 11 patients were outliers. As we checked, the missing values can cause an effect on the analysis result from the obtained data by removing outliers. We found missing values were within 9% in some variables. Therefore we considered the missing values in this analysis. As we considered the fact that there are few variables that contain missing values out of 51 variables, missing percentages were less than 9%, and there wasn't much data, we measured that substitution of data containing missing values will improve the reliability, instead of exemption, therefore, we replaced it by median. According to classified data of 289 patients, the age distribution showed the most at 20s and 30s; 8 patients in teens; 184 in 20s; 79 in 30s; 13 in 40s; and 5 in 50s. The sex distribution of 208 : 81 (male : female) patients showed that male patients greatly outnumbered female patients. The medical examination questionnaire for this study had 51 items, including headache; migraine; muscular or arthritic pain; facial flushing; gum bleeding; heart palpitation; nosebleed or easy bruising; stomatitis; addiction to tobacco and/or coffee; halitosis; cold; seborrheic scalp and skin; hair loss; dry hair; uredo; dry skin; hypotension; hypertension; diabetes; hyperlipidemia; weight loss; cramps; cold sweat and perspiration disorders; cold and heat characteristics; constipation; cold limbs and extremities; gray hair; general, chronic, morning and afternoon fatigue; drowsiness; insomnia and other sleep disorders; vertigo on standing up; xerophthalmia; memory and concentration problems; low vigor; depression; anxiety; irritation; sensitivity to smoke, food ingredients, and chemicals (perfume and detergent); nausea, food allergy, diarrhea/irritable colon syndrome; abdominal swelling; chronic stomach ache; and indigestion. The validation data was obtained from 96 patients through the identical process above (Table 1).
2. Analysis for Chief Complaints
This study used parametric statistics because the questionnaire was related to chief complaints. By using an interval scale, we constructed 51 items with responses scaling from 1 to 10. We measured the degree of symptoms' pain by classification into 10 grades according to hair loss secondary symptoms. The degree of pain was assigned values from 1 to 10, depending on the pain experienced by the 300 patients who visited our clinic. Pain degree "1" meant severe pain and "10," normal cases without pain. These categories were clearly explained by expert to the patients prior to survey. We created statistical models through investigation of the relationship between hair loss and the characteristics of severe hair loss patient in the questionnaire that are classified with "normal" and "severe" to distinguish between patients to infer the correlation between the medical questionnaire items and hair loss. The analysis was performed for 289 patients. The graph frequency was set to 5 and based on the frequency, we classified the patients as 1 (score 1-4) to 'severe' and 0 (score 5-10) to 'normal'. The result appeared severe and normal as 141 and 148 respectively. We used logistic regression and decision tree by using SAS Enterprise Miner ver. 4.3 (SAS Institute Inc, Cary, NC, USA).
The Decision Tree in this study is one of the effective data mining methods and commonly used for classification or prediction. It is because that unlike a nerve network and discriminant analysis method, the decision tree can show rules more clearly underlying application result. Decision Tree has various algorithms and CART, CHAID, C4.5, QUEST are common. In this study, we measured binary splitting as the most appropriate method, since the objective variables were categorical data and there was small amounts of data. Therefore we used CART algorithm based on Gini coefficient in this study. Also, we limited the depth of tree as 3-depth to reduce the misclassification rates that appear when the depth of decision tree is getting deeper by using binary splitting. In addition, all the methods relied on the analysis of all 51 variables at a significance level of p < 0.05.
III. Results
1. Category Analysis Through t-scores
Frequency analysis of physical symptoms were analyzed by selected items, including skin problems, dry mouth, numb and cold limb extremities, heat, dizziness and paleness, chronic fatigues, dermatitis, and drinking and smoking in 26 items referenced by Cornell Medical Index in previous research of Kim and Jeoung [18]. The 26 items were similar to our classification except for the dry hair item in this study.
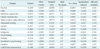
Through effect t-scores of items by the regression node, we found the following items to be most associated with hair loss, in successive order: dry hair > cold > seborrheic scalp and skin > chronic stomachache > addiction to tobacco and/or coffee > abdominal swelling > anxiety > nausea > indigestion > facial flushing > halitosis > nosebleed or easy bruising > irritation > cold limbs and extremities (Table 2). However, we deem that 3 items (nosebleed or easy bruising, irritation, and cold/heat) were not significant factors (p < 0.05) and are not relevant to hair loss; their p-values decreased as the effect t-scores decreased. The categories cold, chronic stomachache, abdominal swelling, halitosis, and irritation seemed to affect hair loss to a greater extent and were less associated to hair loss, with positive value of estimates because of a generally high level of respondents. Thus, as the absolute value of effect t-scores is large, meeting a significant level of p < 0.05 categories, like dry hair, seborrheic scalp and skin, addiction to tobacco and/or coffee, anxiety, nausea, indigestion, and facial flushing are judged to be relevant to hair loss. When examining the odd ratio of these items, the dry hair indicates 0.658 which means that when the units of dry hair increased by 1, the chances of it being 'severe' are 0.658 times higher than before. Since the odd ratio of Seborrheic scalp & skin appeared as 0.813, it tells that the possibility of becoming 'severe' rises 0.813 more as a unit of the item risen by 1 and the rest of the items can be interpreted the same. In a previous study [19], seborrheic dermatitis, pimples, and menstrual irregularity were reported to accompany hair loss. However, most of the researches regarding hair loss focus on stress [20], and mental health [21]. In fact previous studies often used t-test and ANOVA analysis which has the limitation of finding a hidden variable because it can't reflect an interaction between the variables as logistic regression and decision tree analysis. However, construction of a model by logistic regression and decision tree analysis through using the data mining technique provides the chance of finding the hidden variable so we can draw differentiated results than previous research.
2. Designing a Model Questionnaire for Prospective Patients
Based on the questionnaire results of the patients reported herein, we determined logistic regression and constructed decision trees to predict a patients' conditions in prospective cases. Through every NONE model, we selected variables' performances in logistic regression. In addition, a profit matrix was applied to determine the optimal value of the classification criteria (cut-off). In the profit matrix, a misclassification table was created based on a threshold value of 50%. The accuracy (78.20%) that criteria hair loss patients when adapt the questionnaire results of new patients onto the constructed model improved relative to that of pre-distribution (47.79%) by applying a new model questionnaire. The result of validation data also consisted 73.96% as accuracy which has a similar result with the existing model. In this case, the C-table which represents misclassification rates according to cut-off value for seek norm value were omitted because we used the criteria value of the program (Table 3).
3. Decision-making Tree
Table 4 is the misclassification table; it uses the profit matrix of a decision-making tree with a reference to criteria value at a threshold of 50% for classification thus obtained. With the 50% threshold, accuracy (81.31%) improved from pre-distribution (47.79%) with a record that is higher than accuracy of Logistic regression of 78.20%. The findings of validation data also had an accuracy of 78.13% and incur similar outcome with previous model.
The result obtained through the decision-making tree for hair loss patients' chief complaints explained in Figure 1. Based on the criteria of the decision-making tree, values in the dry hair category were set to 6, and seborrheic scalp and skin, drowsiness, cold, addiction to tobacco and/or coffee were classified successively. Results from classification 3 times showed that more than 70% of "severe" patients and "normal" patients were classified at the third node. This ensures that the above 5 categories can classify more than 70% of "severe" patients with relevance to hair loss.
4. Judging Models of Logistic Regression and Decision-making Tree
Table 5 depicts the results of 2 models, which show that accuracy by the decision-making tree is superior to that derived through logistic regression.
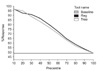
In addition, Figure 2 describes a ROC curve that evaluates performance of models with sensitivity, the possibility of patients' diagnosis test results come as positive, when patients have the disease, on the vertical axis and specificity on the horizontal axis. While better performance is located above the diagonal line, ROC curves are located higher than in the decision-making tree curve. Figure 3 is a response chart of the 2 models. The horizontal axis is the random response rate (48.7%) prior to modeling. The decision-making tree model, regarded as a good model, shows a response rate of 90.70% among top 30% patients.
As a result, the logistic regression model consisting of 14 variables and effect t-scores for each variable was obtained. It is expected to predict the state of hair loss from regression results of the questionnaire for new patients through the "severe" scoring options. Items affecting hair loss can be determined from effect t-score values. We created a tree with leaf = 9 and depth = 4 using the Classification and Regression Trees method (based on separation of Gini coefficients) by selecting the most significant variables for classification of "severe" category for patients at each stage. The decision tree model will also be able to predict the state of new hair loss patients and predict significant items associated with hair loss by considering classification criteria at each stage.
IV. Discussion
This study was based on results from a questionnaire on symptoms of 300 patients who visited the alopecia clinics. To analyze chief complaints of hair loss patients, we used the questionnaires results from 289 individuals; 11 patients had outlier values. Missing values were replaced by the median in the analysis. Analysis showed a level of significance p < 0.05 in 11 items analyzed by the NONE model, including dry hair, cold, seborrheic scalp and skin, chronic stomach ache, addiction to tobacco and/or coffee, abdominal swelling, anxiety, nausea, indigestion, facial flushing, and halitosis. Furthermore, through the effect t-scores obtained by the regression node, items with positive values are less related to hair loss because we judged that the categories of cold, chronic stomach ache, abdominal swelling, bad breath, and irritation are given high scores by the respondents. However, the items that are generally interpreted to be related with hair loss to a greater extent tend to show scores higher than normal. This study shows that 7 categories-dry hair, seborrheic scalp and skin, tobacco and/or coffee addiction, anxiety, nausea, indigestion, and facial flushing-are related to hair loss. In order to ensure the reliability of these results with the logistic regression model and decision-making tree, model assessment was conducted to ensure reliability by deploying the ROC curve and drawing response rate of 90.70% from top 30% patients in the decision-making tree. The questionnaires that have attracted less attention so far have been designed using logistic regression and decision-making trees by data mining. Both models derived improved response rate and significant questionnaire items that are highly associated with alopecia. This study foreshows the secondary symptoms of patients of alopecia by applying the data mining technique and such model questionnaires, it will be possible to predict when a patient should be referred for medical treatment and consultation through the application of the model questionnaire for patients; this will contribute to enhancing patient satisfaction resulting from customized treatment. The data mining technique is not complex, relatively easy to learn and has high utilization compared to the traditional statistic technique [10]. The characteristics or complaints correlated with alopecia as determined from our analysis are relevant and can form the foundation further research on this pertinent aspect. However, this study had certain limitations: it dealt with patients in progress of alopecia. Thus, it is difficult to distinguish the examined results from perfect secondary symptoms. In-depth, extensive research based on epidemiological investigation together with blood and hormone tests in connection with clinical data will contribute to earlier treatment and prevention of alopecia.





 XML Download
XML Download