

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
In recent years, supply has failed to keep up with continuous increases in the demand for emergency medical services [1], which has resulted in problems with overcrowding in Emergency Departments (ED) [2-4]. ED overcrowding has been shown to affect not only patient satisfaction, but also the quality of treatment and prognosis [5-8]. A variety of measures have been taken thus far to address this ED crowding problem [9-11], including staff supplementation, expansions of beds and spaces, diversification of test equipment, the establishment of walk-in clinics for the treatment of light illnesses, hallways, operation of observation units, and allocations of staff and resources according to demand [12,13]. Several studies concerning demand forecasting for allocation of staff and resources have been already been conducted [14-16]. In the emergency medical services field, Spencer et al. previously attempted to forecast demand in the ED using a variety of time series analysis methods [17], and Sun et al. [18]. forecasted the numbers of daily patients in individual ED by considering multivariate factors. Lee et al. [19] employed multiple linear regressions to analyze the factors affecting the number of patients visiting ED in Korea. However, thus far, no studies have been conducted regarding forecasts of the daily numbers of patients visiting ED.
The principal objective of this study was to construct a model by which the number of patients visiting a regional emergency center per day could be predicted, considering calendar and weather data using a moving average, univariate seasonal auto-regressive integrated moving average (SARIMA) and multivariate SARIMA; these models were compared and evaluated.
II. Methods
1. Data Sources
This study was conducted according to a retrospective study design that utilizes a dataset extracted from a tertiary hospital information system (HIS) database. The data utilized for analysis include 189,511 events involving patients who visited the ED from January 2007 to March 2009, excluding their identities (names and hospital numbers). The data for the first two years (Jan. 2007 to Dec. 2008) were used to construct the demand forecast model, whereas those from the past three months (Jan. to Mar. 2009) were used to evaluate the model. Weather data were acquired from the weather agency's website [20].
2. Ethical Consideration
This study employed the summed numbers of patients visiting the ED per day, and utilized no identifications or patients' personal information. Therefore, this study was not subject to review by the Institutional Review Board.
3. Data Preprocessing and Variable Selection
The daily number of patients visiting the ED was employed as a dependent variable, whereas information including the month, day of the week, quarter of the year, holidays, Chuseok [Y/N], seasons, weather factors [20] (average temperature, minimal temperature, maximal temperature, temperature gap, rain [Y/N], snow [Y/N], air-velocity, relative humidity, and yellow dust [Y/N]) were employed as independent variables (Table 1).
The number of patients visiting the ED per day was calculated by counting the number of visiting patients from midnight to the following midnight. Holidays include public holidays and Sundays. Weekdays immediately following a holiday and Saturdays are defined as "After Holiday". Chuseok, which differs significantly from other holidays, is classed as a separate variable. Quantities of precipitation exceeding 10 mm, which ordinary people tend to regard as a significant amount of rain, was the threshold for raining". The operational definition for "snowing" in this study was as abundance of piled-up snow, which again exceeds the general notion of "snowing".
4. Modeling Technique
For this study, the moving average method, the univariate SARIMA model, and the multivariate SARIMA model were used, among other models relevant to the time series analysis method. The moving average method [21], which is known to be the simplest of the forecasting methods, utilizes past time series data (yearly, monthly, quarterly) to calculate the arithmetic mean. Its principal advantage is in its capacity to remove irregular changes or seasonal factors with relative ease. The seasonal ARIMA model [18,19] is an expanded form of the ARIMA, which allows for seasonal factors to be reflected. Unlike the moving average, the trend of time series and the seasonal trend are removed to achieve normality prior to forecasting. The SARIMA model consists of the following: 1) auto-regression; 2) difference; and 3) moving average, and is represented as SARIMA(p, d, q)(P, D, Q), in which (p, d, q) represents the non-seasonal part and (P, D, Q) represents the seasonal part. S represents the length of the seasonality. The p, d, q or P, D, Q represents the auto-regression, difference, and moving average, respectively. The SARIMA model is known to be effective when the components of a time series change rapidly over time, and this model has proven useful in the forecasting of short-term volatility. Unlike the univariate SARIMA model, the multivariate SARIMA model [18] adds an explanatory variable to the SARIMA model, which illustrates the manner in which an alteration in the variable can influence the dependent variables. In this study, the number of patients visiting the ED daily was employed as a dependent variable, and the calendrical and meteorological information are utilized as independent variables for the construction of the forecasting model. The SPSS Time Series Modeler (SPSS ver. 15.0; SPSS Inc., Chicago, IL, USA) is used in the construction of the forecasting model and the comparisons.
5. Model Evaluation
In order to compare the adequacy and performance of the constructed models, residual analysis [22] was conducted and the Akaike Information Criterion (AIC) [23], Bayesian Information Criterion (BIC) [24], and Mean Absolute Percentage Error (MAPE) [17] are calculated. Residual analysis is employed in the time series model to determine whether or not white noise exists in the residuals, which are the differences between the predicted and observed values. If the residuals move randomly centering on 0 (the average of the residuals) in the time series diagram and the autocorrelation function diagram of the residuals and the deviation is constant, while the autocorrelation function falls within the confidence interval for all time differences, then the residuals are statistically independent; thus, we can be assured of the fitness of the model.
As the SARIMA model does not distinguish clearly between the partial auto-correlation function (PACF) and the auto-correlation function (ACF), it compares the AIC and BIC values from forecasting models and selects the one with the smallest value as the final forecasting model. MAPE represents the relative scale of the forecasting error between the forecasted value, which is a series variable, and the observed value; the smaller the error, the more accurate the forecast is.
III. Results
Data collected from the 2007-2008 period was employed in the development of the model used to forecast the daily numbers of patients visiting the ED. The total number of patients who visitied the ED during that period was 169,375, with an annual average of 84,668 and a daily average of 232. Chi-square tests were in order to ascertain whether any significant differences could be detected between the two datasets, and no significant differences were detected at a confidence interval of 95% (Table 2).
The time series diagram shows that the number of patients per day begins to increase on Saturday and peaks on Sunday, and then begins to decrease on Monday and stays low until Friday, thus describing a 7-day cycle (Figure 1).
That diagram also demonstrates that the number of visiting patients over time trends upward. The 1st seasonal difference was applied to remove the seasonal trend. As a consequence, the time series diagram suggests a stationary time series, in which the mean and deviation could not be observed clearly (Figure 2).
Three models-the MA(2) for the moving average model, SARIMA(1,0,1)(0,1,1)7 for the univariate SARIMA model and SARIMA(1,0,2)(0,1,1)7 for the multivariate SARIMA model--were constructed using the SPSS Time Series Modeler. Parametric estimations using the maximal likelihood method showed that only the variables Chuseok, seasons (spring, summer, fall, and winter), average temperature, and rain could be selected as explanatory variables for the multivariate SARIMA model (Table 3).
Residual analysis for the purpose of determining the adequacy of the constructed models shows that the univariate SARIMA model and the multivariate SARIMA model, respectively, have an average of residuals that moves randomly but us centered on 0, and that the constant deviations and autocorrelation functions fall within the confidence interval, thereby indicating that the residuals are independent and fulfill the 'white noise' criterion.
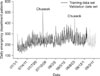
The diagram that compares the forecasted and observed values over three months in the three forecasting models shows that the MA(2)'s forecast virtually displays the mean of the observed value, thus reflecting its inadequacy as a prediction model (Figure 3).
On the contrary, the SARIMA model exhibits a pattern of change similar to the observed values. Superficially, it is difficult to distinguish between the univariate and multivariate SARIMA models. The AIC and BIC values, which compare the adequacy of the models, are better in the ARIMA model than in association with the moving average method, with the SARIMA(1,0,2)(0,1,1)7 model evidencing more adequate results than the univariate SARIMA model (Table 4). A MAPE comparison of the accuracy of each model's forecasting ability demonstrates that the MA(2) models scored a 12.9%, the univariate SARIMA(1,0,1)(0,1,1)7 model scored 7.8%, and the multivariate SARIMA (1,0,2)(0,1,1)7 model scored 7.4%, thus identifying the final model as the most accurate forecasting model (Table 4): the normalized BIC values for the training and test data were also presented for comparisons.
IV. Discussion
In this study, three models are developed to forecast the number of patients visiting an ED per day: [A] Moving average model: MA(2), [B] univariate seasonal ARIMA model: SARIMA(1,0,1)(0,1,1)7, and [C] multivariate seasonal ARIMA model: SARIMA(1,0,2)(0,1,1)7. A comparison of the goodness of fit of the three forecasting models shows that only the final two models have residuals that fall within the confidence interval.
A comparison of the models' forecasting accuracy shows the multivariate SARIMA model (SARIMA(1,0,2)(0,1,1)7) to be the most accurate, with a MAPE of 7.4%. The two SARIMA models have a MAPE of less than 10%, thereby suggesting a high degree of accuracy. As the SARIMA models exhibit autocorrelation and the capacity to account for seasonality, they also tend to evidence accuracy higher than the moving average. It appears that the multivariate seasonal ARIMA model can forecast the number of visiting patients more accurately than the univariate model, as it incorporates explanatory variables that affect that number (Chuseok, seasons, average temperature, and absence or presence of rain).
Batel et al. [25] previously demonstrated that the number of visiting patients peaks on Monday and continues to decrease until Sunday, whereas Lee et al. [19]. demonstrated that the number of patients per day begins to increase on Saturday and peaks on Sunday, and then begins to decline on Monday and remains low until Friday, exhibiting a 7-day cycle and a seasonal trend. This may be attributable to differences in the medical environments. Batel et al. [25]. employed walk-in-clinics that operate for 15.5 hours over the entire week. In this study, the number of patients visiting the ED rises on Sundays and public holidays such as Seollal and Chuseok. This is because outpatient treatments are all closed on holidays, which means that the ED does double duty.
Lee et al. [19] identified a weak correlation among the maximal, minimal, and average temperature of the day and the number of visiting patients, and reported no differences in the number on rainy days and non-rainy days. The same is true for snowy days and non-snowy days. Spencer et al. [17] also argued that weather has only a minimal effect on number of patients who visited an ED. This study, however, shows that the multivariate SARIMA model that incorporates multiple weather factors generates the optimal results, thus suggesting that weather, and rain in particular, affects the numbers of visiting patients. Considering that patients in Korea consist of the following three types -1) those in an emergency situation, who require immediate treatment, 2) non-emergency patients who seek treatment on holidays or at night, and 3) non-emergency patients who seek outpatient treatment without a doctor's reference- it can be inferred that the non-emergency patients are impacted most profoundly in this situation. In fact, Hwang et al. [14] has reports that 2,276 out of 4,273 new patients (53.3%) obtain treatment at an ED. As a consequence, considering the number of non-emergency patients who visit the ED, it is necessary to take into account weather factors when constructing demand forecasting models for emergency medical centers.
It will also be necessary to develop a variety of demand forecasting models that reflect local environments, since the studies conducted thus far have failed to take into consideration local medical systems, social and cultural backgrounds, and the relevant geographical factors.
In conclusion, as the result of our comparison of the three constructed forecast models, it was determined that the multivariate SARIMA model that incorporates explanatory variables was the most appropriate for forecasting the daily number of patients visiting the ED; this model appears to reliably and accurately forecast the number of patients admitted to the ED per day. The results of this study demonstrated that weather information, particularly temperature and rain (or the absence there of), should be considered when attempting to predict the daily volume of ED patients. The proposed prediction model can be used to forecast the daily patient volume in ED, and preparing for the previously mentioned ED crowding problems regarding the allocations of staffs and resources. More detailed prediction models related to medical demands in ED on resources and easement of overcrowding can be achieved from the proposed model via more departmentalized and processed variables that affect staff supplementation, space shortages, and the diversifications of test equipments.






 XML Download
XML Download