

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Tenofovir disoproxil fumarate (TDF) is the preferred nucleoside reverse transcriptase inhibitor (NRTI) to initially treat human immunodeficiency virus (HIV)-infected patients except pregnant women. TDF was approved by Food and Drug Administration in 2001 to treat hepatitis B virus (HBV) and HIV infection [1]. Tenofovir and emtricitabine (TDF/FTC) are preferred treatment among the NRTIs according to US Department of Health and Human Services (DHHS) and the US International Antiviral Society guidelines [23].
Despite continuous use of antiretroviral therapeutics and the development of new drugs, kidney disease is a critical problem in HIV-infected patients [4]. Proteinuria, interstitial nephritis, renal tubular damage, and nephrolithiasis have been detected as renal complications of HIV infection [5]. Comorbidities, such as diabetes mellitus, hypertension, hepatitis C virus (HCV) co-infection, and specific antiretroviral drug use, are risk factors for kidney disease, which causes atherosclerosis and increases mortality rates [67]. Nephrotoxicity can appear either during long or short-term use of TDF. TDF-induced nephrotoxicity is reported in about 15% of patients treated with TDF for 2-9 years [8]. Previous studies have reported several risk factors for TDF-induced nephrotoxicity, including high basal serum creatinine (Cr) level, concomitant use of nephrotoxic drugs, low body weight, old age, and low CD4+ T cell count [9]. It is presumed that proximal tubule damage, diabetes insipidus, decreased bone density, and reduced glomerular filtration rate (GFR) could also occur in association with TDF use [10111213]. In addition, combinations of protease inhibitors (PI), such as atazanavir (ATV) or lopinavir (LPV), can an additional decrease in GFR, compared to a combination with a non-nucleoside reverse transcriptase inhibitor (NNRTI), such as efavirenz (EFV) [1415].
In this study, we investigated the incidence and clinical characteristics of an acute increase in serum Cr level more than 1.5 mg/dL during TDF/FTC-based highly active antiretroviral treatment (HAART) in HIV-infected patients.
Materials and Methods
1. Study design and subjects
This retrospective study was conducted using the medical records of patients treated with HAART including TDF/FTC at Kyungpook National University Hospital between February 1, 2010 and April 30, 2014 (Fig. 1). Exclusion criteria were too short treatment duration (<6 days), lack of blood chemistry or other blood laboratory data, and the patient's medical records could not be reviewed. The patients were divided into three groups of TDF/FTC + ritonavir-boosted PI (PI/r) (group 1), TDF/FTC + NNRTI (group 2), and TDF/FTC + integrase strand transfer inhibitors (INSTI) (group 3) and three PI/r subgroups of TDF/FTC + LPV/r (subgroup 1), TDF/FTC + ATV/r (subgroup 2), and TDF/FTC + darunavir (DRV)/r (subgroup 3).
The clinical factors investigated included age, sex, period of treatment and follow-up, treatment failure rate, comorbidities, such as syphilis, hepatitis C, hepatitis B, hypertension, diabetes mellitus, thyroid disease, concomitant medications [anti-tuberculosis drugs, ganciclovir (GCV) or valganciclovir (VGCV), analgesics, antipsychotic drugs, trimethoprim/sulfamethoxazole (TMP/SMX)], CD4+ T cell counts, HIV-1 RNA levels, blood urea nitrogen (BUN), and serum creatinine (Cr). Beginning levels and peak levels of serum BUN and serum Cr were measured in each group and compared. The acute increase more than 1.5 mg/dL in serum Cr level was used as an indicator of nephrotoxicity.
2. Statistical analysis
Patients' characteristics were described as mean [SD] for normally distributed continuous variables, median [IQR] for non-normally distributed continuous variables, and percentages for categorical variables. We evaluated differences among three groups via analysis of variance (ANOVA) or Kruskal-Wallis H test for continuous variables, and chi-square test for categorical variables, as appropriate. Statistical analyses and data sorting were performed using SPSS ver. 22.0 (SPSS Inc., Chicago, IL, USA). A P-value of less than 0.05 (two-tailed) was considered statistically significant.
Results
1. Baseline characteristics and concomitant medications of the patients treated with TDF/FTC-based HAART
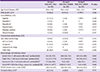
Among the 205 patients, 69 were excluded. Thus, 136 patients were included in the final analysis. The distribution of patients was 91 in group 1, 20 in group 2, and 25 in group 3 (Fig. 1). Table 1 shows the demographic data of the study groups. No differences in the distributions of comorbidities for syphilis, hepatitis C, hepatitis B, hypertension, diabetes mellitus, and thyroid disease were found among the groups (Table 1). A considerable number of patients were taking other medications besides the antiretroviral drug, including were anti-tuberculosis drugs, GCV or VGCV, analgesics, antipsychotic drugs, and TMP/SMX, but no significant differences were found among the groups (Table 1). All three groups showed significant increases in CD4+ T cell counts. Initial HIV RNA level was significantly lower in group 3 [P=0.006] (Table 1).
2. Changes in renal function and the incidence of nephrotoxicity of the three TDF/FTC-based HAART groups
Changes in serum Cr level were detected during TDF/FTC-based antiretroviral therapy in group 1 (0.12 [0.06, 0.24] mg/dL), group 2 (0.08 [0.02, 0.13] mg/dL), and group 3 (0.16 [0.07, 0.27] mg/dL) [P > 0.05] (Table 2). Four patients (all in group 1) had serum Cr levels more than 1.5 mg/dL. The overall incidence of serum creatinine increase more than 1.5 mg/dL was 2.8 cases per 100 patient-years, and that of TDF/FTC + PI/r group was 4.0 cases per 100 patient-years.
3. Baseline characteristics and concomitant medications of patients treated with TDF/FTC + PI/r patients subgroups
The distribution of patients in the TDF + PI/r subgroups was: 23 in subgroup 1, 18 in subgroup 2, and 50 in subgroup 3. The demographic data are shown in Table 3. The distributions of comorbidities among the subgroups were not different. About 70-98% of the study subjects took medications other than an antiretroviral drug, including anti-tuberculosis drugs, GCV or VGCV, analgesics, antipsychotic drugs, and TMP/SMX. No difference was found among the subgroups except initial CD4+ T cell count (Table 3). The number of CD4+ T cells at the beginning of treatment was significantly higher in subgroup 2 (median 346/mm3, IQR [238, 677]) that that in the other subgroups.
4. Changes in renal function and the incidence of nephrotoxicity in the three TDF/FTC + PI/r subgroups
The changes in serum Cr levels during TDF/FTC + PI/r-based HAART were 0.11 [0.05, 0.22] mg/dL in subgroup 1, 0.15 [0, 0.34] mg/dL in subgroup 2, and 0.12 [0.06, 0.23] mg/dL in subgroup 3 [P > 0.05] (Table 4).
All four patients whose serum Cr was > 1.5 mg/dL during treatment were in the TDF/FTC + PI/r group (one in subgroup 1 and three in subgroup 2). Initial serum Cr level was lower in subgroup 3, but there were no statistical differences of peak serum Cr levels and increment of serum Cr levels during HAART among three groups (Table 4). No case in subgroup 3 had an acute increase in serum Cr more than 1.5 mg/dL. The clinical characteristics and clinical course of these four patients was summarized in Table 5. The time interval from start of HAART to occurrence of acute serum Cr increase was from 210 to 662 days. Serum Cr levels of all four patients were recovered to the level less than 1.5 mg/dL after HAART regimen change from TDF/FTC + PI/r to abacavir/lamivudine + INSTI.
Discussion
In this study, changes in serum Cr levels in groups classified according to the drug used with TDF, such as PI/r, NNRTI, and INSTI was evaluated. First, four patients (2.9%) in our study had serum Cr levels that increased more than 1.5 mg/dL during HAART. Other study that treated 10,000 HIV-infected patients with TDF and monitored the increase in serum Cr found that 2.2% of cases showed baseline serum Cr more than 0.5 mg/dL and 0.6% increased more than 2.0 mg/dL [8], which was similar to our results. Second, the four patients whose serum Cr increased more than 1.5 mg/dL were administered both TDF and a PI/r drug. Of them, one was in the LPV/r group and three were in the ATV/r group. This finding shows that the risk of deteriorating kidney function may increases when TDF is applied with PI/r. Goicoechea et al. reported that changes in GFR of 146 patients were observed among three groups - TDF + PI/r, TDF + NNRTI, non-TDF combination regimen [14]. No difference was found among the three groups from weeks 1 to 24. However, the TDF + PI/r group revealed the greatest decreased in GFR on week 48, compared with that of the TDF + NNRTI groups [P = 0.04], similar with our study results.
Various studies have reported the relationship between TDF use and kidney diseases. In a retrospective study conducted on 1,647 cases of initial antiretroviral treatment, a more acute decrease in GFR was noted in the TDF compared to that in the non-TDF group [16]. In another study, more cases of abnormal proximal tubule functioning and decreased GFR occurred in patients who had been taking TDF for > 24 months [1718]. TDF is toxic to mitochondria, which may result proximal tubule damage that prevents resorption of filtered phosphate, potassium, amino acids, and glucose [19]. The risks of proteinuria, a sharp decrease in kidney function, and chronic kidney disease increased annually by 34%, 11%, and 33% respectively, in 10,000 patients infected with HIV and treated with TDF [17]. In another prospective cohort study, patients administered a combination of TDF and LPV/r or ATV/r showed a decrease in GFR compared to those administered TDF and EFV. Of the combined PI groups, the ATV/r group showed the poorest result [1520]. Ryom et al. reported a study of 22,603 patients whose pre-treatment estimated glomerular filtration rate (eGFR) was > 90 mL/min. Decreases in eGFR (20 mL/min in 2.1% and 60 mL/min in 0.6% of cases) were observed when the patients were treated with TDF, ATV, LPV/r, abacavir (ABC) and another PI/r [21]. Sustained use of LPV/r could be related with chronic deterioration in kidney function [14152122].
Increased serum Cr, concomitant medications likely to cause toxicity, underweight, older age, the duration and dose of TDF, and a low CD4+ T cell count were known as major risk factors for nephrotoxicity caused by TDF [9]. However, in our study only two patients were more than 60 year-old, the others were not old. Two patients (case 3 and 4 in Table 5) had taken atorvastatin as concomitant medication, which had been well known as the potential drug developing rhabdomyolysis, resulting acute renal injury. Therefore, concomitant statin medication in boosted PI-based HAART patients might need more precaution by clinicians to prevent occurrence of TDF-related acute renal injury.
Because relatively high incidence of adverse effects including nephrotoxicity has been reported in PI/r regimen containing TDF, the primary regimens for the initial HAART treatment of HIV-infected patients were changed in the newly issued DHHS guidelines published in April 2015: the four regimens with INSTI; dolutegravir (DTG)/ABC/lamivudine, DTG + TDF/FTC, EVG/COBI/TDF/FTC, RAL + TDF/FTC, and one regimen with PI/r; DRV/r + TDF/FTC. ATV/r + TDF/FTC regimen, which was the primary regimen before 2014, was changed to a secondary regimen [23].
spectively, therefore we could not sufficiently assess the clinical indicators showing the development of kidney toxicity, and we had to use serum Cr level only. Serum Cr is produced by skeletal muscles. Most HIV-infected patients have an abnormal muscle mass compared to that of a healthy subject; thus, more caution is required for interpretation [24]. Other previous reports investigating renal function decline prospectively had used an estimated glomerular filtration rate (eGFR) [6791415172025], albuminuria [6], proteinuria [24], urine protein/creatinine ratio [8], and the rate of creatinine clearance (CrCl) [24] as the indicator of decrement of renal function. However, because of retrospective nature of our study, we could not evaluate these markers that had been known as more predictive and accurate indicator. Also, the study group was limited to patients from one hospital, and the total number of patients was small, which also affected the results assessment. But, our results may be significant because this is the first Korean report on TDF-induced nephrotoxicity.
In conclusion, this study results showed that TDF containing PI/r regimen might be related with relatively higher rate of acute serum Cr elevation during HAART. Therefore, more caution might be needed when clinicians treat HIV-infected patients with TDF containing PI/r regimen, especially using ATV/r or LPV/r with TDF.





 XML Download
XML Download