

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
During the last twenty years, the development of antiretroviral drugs and the use of highly active antiretroviral therapy (HAART) have dramatically reduced mortality among patients infected with human immunodeficiency virus (HIV). The success of ART has led to HIV becoming a chronic disease [123]. Therefore, the period of medication of HIV infected patients has been prolonged, and adverse events and adherence have become more important. Taking regular medication is important for the treatment of HIV, because poor adherence plays a major role in the emergence of resistance and treatment failure. Poor adherence to therapy affects the viral load reduction and the recovery of CD4+ lymphocytes, and it is also strongly associated with disease progression and mortality [456]. Various factors influence treatment adherence, including medications, patient factors, and socioeconomic factors. Patient sex, age, economic status, active substance abuse, level of education, the lack of family and social support, neurocognitive function, and psychiatric problems are important socioeconomic and patient factors. The medication-associated factors include side effects, pill burden, type of regimen, drug interactions, ease of storage, and food requirements [7]. Tolerability is also an important factor affecting treatment adherence.
The efficacy of ART has improved, and the adverse effects of antiretroviral drugs have been reduced. However, adverse events during ART are the most important determinants of adherence. With virologic failure, tolerability failure, defined as the permanent discontinuation of antiretroviral drug treatment as the result of an adverse event, was investigated as a clinical outcome parameter in a previous study [8]. Therefore, we investigated the switching rate and the adverse effects of the first ART. We also evaluated the regimen classes and antiretroviral drugs associated with changes in the first ART. Additionally, we investigated which antiretroviral drugs within these classes were most likely to cause regimen switching.
Materials and Methods
1. Subjects and study design
A retrospective study was performed by reviewing the medical records of HIV-infected patients who started their first HAART at the Kyungpook National University Hospital (KNUH), a tertiary teaching hospital in South Korea, between January 1, 2011 and July 30, 2014. Patients who fulfilled the following criteria were included in this study: (1) age ≥18 years; (2) first ART initiated at the KNUH; (3) follow-up for ≥12 weeks. Patients fulfilling the following criteria were excluded from this study: (1) age <18 years; (2) treatment for post-exposure prophylaxis; (3) pregnancy; (4) previously treated with ART and commencing second-line treatment.
Using medical records, we examined why patients switched from the first ART regimen, the date when treatment was started, and the last follow-up date of the first ART regimen. We calculated the period of the first ART regimen as the time difference between these two dates. Among the patients who met the inclusion criteria, the patients who switched their first ART regimen because of the side effects of other drugs were excluded from this study. If the reason for switching the first ART regimen was side effects of antiretroviral drugs, we investigated adverse effects that cause ART switching. The collected adverse effects were headache, nausea or upper abdominal pain, rash, headache, dizziness, diarrhea, elevation of aspartate aminotransferase (AST) and alanine transaminase (ALT), and hyperbilirubinemia.
The patients were classified into three groups, depending on the initial treatment regimen: a protease inhibitor (PI)-based regimen group; a non-nucleoside reverse transcriptase inhibitor (NNRTI)-based regimen group; and an integrase inhibitor (II)-based regimen group. The PI-based regimen group included the following drug combinations: co-formulated tenofovir/emtricitabine (TDF/FTC) + ritonavir-boosted darunavir (DRV/r); TDF/FTC + ritonavir-boosted atazanavir (ATV/r); co-formulated abacavir/lamivudine (ABC/3TC) + DRV/r; ABC/3TC + ATV/r; 3TC + ABC + ATV/r; ABC/3TC + ritonavir-boosted lopinavir (LPV/r); 3TC + ABC + LPV/r; co-formulated lamivudine/zidovudine (3TC/ZDV) + LPV/r. The NNRTI-based regimen group included the following drug combinations: TDF/FTC + efavirenz (EFV); LPV/r + EFV; 3TC + ABC + EFV; TDF/FTC + rilpivirine (RPV). The II-based regimen group included the following drug combinations: TDF/FTC + raltegravir (RAL); co-formulated elvitegravir/cobicistat/emtricitabine/tenofovir (EVG/COBI/FTC/TDF). We compared the maintenance of the first ART regimen according to the time between these groups. In addition, we compared the maintenance of therapies containing individual drugs within these ART classes. We excluded patients who changed their initial antiretroviral regimen because of other reasons other than adverse effects. One study population was referred to as the adverse effect-associated regimen switching group, while the original study population was considered as all-case regimen switching.
2. Definitions
Diarrhea was defined as passage of liquid or unformed stool which frequency is more than three times per day [9]. Elevation of AST and ALT were defined as the case that was more than twice the upper limits of normal (ULN; AST: 36 IU/L, ALT: 41 IU/L) [101112]. Hyperbilirubinemia was defined as the case that was higher than ULN (ULN; total bilirubin: 1 mg/dL) [1112]. Patients who meet the following diagnostic criteria were defined as diabetes; HbA1C ≥6.5% or fasting plasma glucose ≥126 mg/dL or 2-hour plasma glucose ≥200 mg/dL [913]. Presence of other adverse effects such as rash, upper abdominal pain or nausea, headache and dizziness was adopted by reviewing medical records.
3. Statistical analysis
Statistical analyses were performed using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA). The survival analysis with log rank test was used to analyze differences in maintenance rate of the first antiretroviral drug regimen between the regimen groups and between individual drugs within these groups. The
frequency of the adverse effects of ART regimens was analyzed by multiple response data analysis. P-values < 0.05 (twotailed) were considered statistically significant.
Results
During the study period, 137 HIV-infected patients started ART. Ninety-eight of these were prescribed PI-based regimens (71.5%), 26 (19.0%) were prescribed NNRTI-based regimens, and 13 (9.5%) were prescribed II-based regimens (Table 1). Eighty-one patients were maintained on their initial ART regimen throughout the research period. We investigated the frequency of use of each drug. In PI-based regimens, DRV/r was used in 29 patients, LPV/r was used in 33 patients, and ATV or ATV/r was used in 36 patients. In the NNRTI-based regimens, EFV was used in 20 patients, and RPV was used in 6 patients. In the II-based regimens, RAL was used in 8 patients, and EVG/COBI/FTC/TDF was used in 5 patients. TDF/FTC and ABC/3TC were used in 70 and 31 patients, respectively.
Among the 56 patients who switched from their initial ART regimen, 35 patients changed regimens because of the adverse effects of the antiretroviral drugs. The remainder (n = 21) switched because of other reasons. In PI-based regimens, 44 patients were switched from the initial ART regimen. Among these patients, 26 patients (26/44, 59.0%) switched the initial ART regimen because of adverse effects. Within the NNRTI-based regimen groups, 11 patients were switched from the initial ART regimen. Nine (9/11, 81.8%) patients switched from the initial ART regimen because of adverse effects. In IIbased regimens, one patient was switched from the initial ART regimen, but not because of adverse effects (Table 1). In the 26 patients who switched from the initial PI-based ART regimen because of adverse effects, DRV/r was used in 2 patients, ATV or ATV/r was used in 13 patients, and LPV/r was used in 11 patients. All patients who changed the initial NNRTI-based regimen because of adverse effects were prescribed EFV. However, patients who were initially prescribed RPV did not discontinue initial antiretroviral drugs (Table 1).
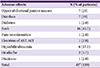
In the 35 patients who experienced adverse effects, 42 cases of overlapping adverse effects were observed. The most common adverse effects included rash (n = 16, 45.7% of patients), upper abdominal pain or nausea (n = 7, 20%), diarrhea (n = 7, 20%), and hyperbilirubinemia (n = 6, 17.1%). Headache and dizziness were observed in 2 patients (5.7% of patients) and 1 patients (2.8%), respectively (Table 2).
The survival curves of treatment regimens are shown in Figure 1. The results of the log rank tests comparing the maintenance rate in these regimen groups for all-cause regimen switching were as follows: PI versus II, P = 0.037; and NNRTI versus II, P = 0.044 (Fig. 1A). The results of the log rank tests comparing the maintenance rate in these regimen groups for adverse effect-associated regimen switching were as follows: PI versus NNRTI, P = 0.384; PI versus II, P = 0.039; and NNRTI versus II, P = 0.019 (Fig. 1B). The groups taking II-based regimens showed higher maintenance rate of the initial antiretroviral regimen than that of PI-and NNRTI-based regimen groups, and this difference was statistically significant. In the NNRTI-based regimen group, frequent switching was observed early in the administration period (Fig. 1A, 1B). The PI- and NNRTI-based regimen groups often switched treatment regimen within 18 months (Fig. 1A). After this time-point, these regimens were maintained without change (Fig. 1A).
The survival curves associated with individual PI-based regimens are shown in Figure 2A. The curves of groups receiving ATV/r and LPV/r showed a steep descent at early time-points and reached a plateau after 12 months. However, the curve for those receiving DRV/r reached a plateau with a gentle descendent. The results of the log rank tests comparing the maintenance rate between PI drugs for all-cause regimen switching were as follows: DRV/r versus LPV/r, P = 0.011; and DRV/r versus ATV/r, P = 0.004. The results of the log rank tests for comparing the maintenance rate between PI drugs for the adverse effect-associated regimen switching were as follows: DRV/r versus LPV/r, P = 0.010; and DRV/r versus ATV/r, P = 0.04 (Fig. 2A). DRV/r was rarely switched due to adverse effects and this difference from other drugs in this category was statistically significant. A within-group comparison of the NNRTI-based regimens showed that RPV had a significantly lower frequency of changes than EFV (P = 0.045 for all-cause regimen switching, P = 0.045 for adverse effect-associated regimen switching) (Fig. 2B).
Discussion
Recently, mortality caused by opportunistic infections in HIV patients has been decreased by the administration of effective antiretroviral drugs. Thus, HIV/acquired immune deficiency syndrome (AIDS) has changed into a chronic manageable disease pattern. Accordingly, new treatment strategies and approaches to patient management are needed to treat these patients [1415]. Treatment adherence reflects the degree of concordance between the recommendation of the doctor and the actions of their patient. This has an important influence on the long-term success of HIV/AIDS treatment. Various factors can degrade adherence and these include the doctor-patient relationship, socioeconomic factors, and medication factors. According to many previous studies, adverse drug effects are one of the main factors leading to reduced adherence [71617181920].
The most common adverse effects of antiretroviral drugs are rash, hypersensitivity reaction, anemia, gastrointestinal discomfort, jaundice, and side effects on the central nervous system (CNS). The gastrointestinal side effects are diarrhea, nausea, and vomiting. These are the major reasons for discontinuation in the early phase of ART [21]. PI drugs can produce severe gastrointestinal adverse effects, while NNRTI and II drugs have fewer of these effects. Comparative studies within PI drugs have shown that ATV/r and DRV/r produced fewer adverse gastrointestinal effects than LPV/r [2223]. Within the NNRTI drugs, RPV produced fewer rashes and adverse gastrointestinal effects than EFV [2425]. CNS adverse effects including insomnia, nightmares, headaches, and dizziness are commonly observed at NNRTI drugs. These tend to appear soon after therapy initiation and mostly improve within 4 weeks. Adverse CNS effects are also associated with II drugs, although to a lesser extent than those observed at NNRTI drugs. A study comparing EFV with RAL showed that RAL caused less adverse CNS effects than EFV [26]. Rash is a common adverse effect that can be caused by many drugs; the main ART responsible for this side effect is NNRTI drug. Rash is observed in 10-17% of patients receiving NNRTI drugs. However, this is mostly mild and was only associated with a discontinuation rate of about 2% [27]. In the present study, the adverse effects causing the first ART switch included rash, nausea, vomiting, and hyperbilirubinemia; this finding was consistent with those of previous studies. However, we found that rash occurred more frequently than adverse gastrointestinal effects. We think that are differences between the severity of adverse effects that lead to ART switching and the frequency of the adverse effects.
We found that NNRTI-based regimens employing RPV showed a lower percentage of discontinuation/continuation over time than those employing EFV. Previous studies have investigated the safety and tolerability of NNRTIs. Monlia et al. [24] reported that the incidence of treatment-related grade 2-4 adverse events was lower for RPV than for EFV (RPV [55/346] versus EFV [108/344], P < 0.0001). The incidence of discontinuation due to adverse events was lower for RPV (6/346) than for EFV (25/344). Cohen et al. [25] reported that the incidence of discontinuation due to adverse events was greater for EFV than for RPV (RPV [9/340] versus EFV [24/338]). Our study also showed that EFV was more frequently stopped early after ART initiation.
Our comparison within the PI-based regimens indicated that DRV/r showed a lower percentage of discontinuation/continuation over time than those involving other PIs. ATV/r was stopped earlier than LPV/r, although this difference was not statistically significant. Orkin et al. [22] reported that DRV/r produced fewer treatment-related adverse gastrointestinal events and less discontinuation due to adverse events. The incidence of hyperbilirubinemia was also lower during DRV/r therapy. Our data in relation to DRV/r were consistent with this report. Molina et al. [23] also reported that ATV/r showed less discontinuation than LPV/r. Treatment-related adverse gastrointestinal events such as diarrhea and nausea were reported less frequently during administration of ATV/r, as compared with than LPV/r; however, rash and hyperbilirubinemia were more apparent with ATV/r than with LPV/r. Hyperbilirubinemia and gastrointestinal problems are the main factors leading to discontinuation of PI-based regimens.
Treatment duration survival analysis showed that II-based regimens had a significantly lower ratio for discontinuation/continuation over time than that of the other treatments. The PI- and NNRTI-based regimens reached a steady state after 18 months. In the STARTMRK study, therapy of individuals in the RAL-based therapy group was stopped less frequently due to adverse events than was that of those in the EFV-based therapy group and the time to discontinuation was significantly longer in the RAL group than in the EFV group (log rank P-value = 0.023) [28]. Similarly, the present study showed that IIbased regimens maintained the initial ART for longer than NNRTI-based regimens.
In a previous comparison of ABC/3TC and TDF/FTC with DRV/r, the TDF/FTC regimen was tolerated more effectively than the ABC/3TC regimen [29]. We also performed survival analyses between TDF/FTC and ABC/3TC. But, survival curves showed cross-over. Therefore, we could not analyze log rank test to compare TDF/FTC with ABC/3TC. In this study, nucleoside reverse transcriptase inhibitor (NRTI) drugs were used as a backbone nucleoside. So, anchor drugs of each NRTI drugs were various. We thought that anchor drugs would influence the result of survival analyses.
There were some limitations to this study. First, this was a retrospective study. Thus, in some cases, we were unable to determine the reason for switching from ART drug treatment. Additionally, we could not evaluate all adverse effects using the Common Terminology Criteria for Adverse Events (CTCAE) criteria. Second, we predicted that tolerability failure was more related to patients' subjective factors than to objective evidences such as the severity of adverse events. Therefore, we defined the adverse effects, including low levels of toxicity, which were lower than those observed in previous studies. Consequently, there were large differences in the frequency of adverse effects compared to those found in previous studies. Third, the size of the overall study population was small and this limited the subgroup analyses. Therefore, future studies should aim to recruit additional patients, facilitating comparisons of the treatment regimens. A further comparative study of RAL and EVG will be required. Fourth, the maximum follow-up duration for the first ART regimen varied. If the duration was similar, the statistical p value would have been different in some comparative arms. Particularly, in the comparison of RPV and EFV, the p value would have been affected. However, our study did identify statistically significant differences between regimen groups and obtained clinically meaningful information about the adverse effects that resulted in regimen switching.
In summary, adverse effects often caused discontinuation of the initial ART. II-based regimens showed better adherence than other regimens. PI- and NNRTI-based regimens were vulnerable to switching at early time-points but tended to stabilize when maintained for over 18 months. It is important to understand, monitor, and treat common adverse events in order to maintain patient adherence and improve outcomes.



 XML Download
XML Download