

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Actinobacillus (Pasteurella) ureae is a commensal of the human respiratory tract and various mammals. It is an organism of low pathogenicity and is a rare human pathogen (1). Only 28 cases of A. ureae infections in humans have been reported since its first description in 1960, including meningitis (2), pneumonia (3-6), hepatitis (7), sepsis (7, 8), conjunctivitis (9), otitis media (10), peritonitis (11), endocarditis (12), chronic bronchitis (13), bone marrow infection (14) and septic arthritis (15). Here, we report the first case, in the medline-based literature, of A. ureae psoas muscle abscess and sepsis in a HBV carrier patient.
CASE REPORT
A 76-year-old male was admitted to the department of internal medicine with fever, lower back pain, and general weakness after suffering from a slip-down injury 25 days before admission while working at his farm. His past medical history was positive for chronic hepatitis B infection, stroke, and hypertension. He had undergone appendectomy and hydrocelectomy. However, he was not a smoker nor drank alcohol.
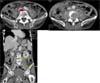
On initial physical examination, he was acutely ill looking and showed confused mentality. His body temperature was 38.1℃, blood pressure was 140/80 mmHg, pulse rate was 96 beats/min, and respiration rate was 20 breaths/min. Positive clinical findings included tenderness and swelling on the lower back. The chest X-ray was unremarkable. The abdominal CT showed L4 vertebral body compression fracture with both psoas muscle abscess (right: 2.7×1.7×1.3 cm, left: 4.3×2.1×2.3 cm) (Fig. 1). Laboratory results were as follows: normochromic normocytic anemia (Hb = 10.2 g/dL, Hct = 30.0%); white blood cell count (WBC), 14.21×109/L (polymorphs, 76.9%; lymphocytes, 9.6%; monocytes, 11.2%; eosinophils; 0.8%); platelet, 427×109/L; erythrocyte sedimentation rate (ESR), 85 mm/h; C-reactive protein (CRP), 12.65 g/L; AST, 279 IU/L; ALT, 142 IU/L; ALP, 198 IU/L; total bilirubin, 0.8 mg/dL; prothrombin time, 20.6 sec (INR=1.88). Other blood biochemistry tests were normal (Table 1). His HBsAg was positive and HBV-DNA was 393,900 copies/mL. The patient was initially treated with intravenous ceftazidime and metronidazole. On the 7th hospital day, the fusion operation of L4-5 vertebral body and incision and drainage was performed. The blood culture was positive for A. urea, which was susceptible to penicillin, amikacin, ampicillin, aztreonam, cefazolin, cefotaxime, ciprofloxacin, gentamicin, and cotrimoxazole. Antibiotics were changed to ceftazidime. Echocardiography showed no vegetation on cardiac valves. A few days after treatment, fever subsided and inflammatory indices such as ESR, CRP, and platelets returned to normal values. Follow up abdominal CT scan after 25 days of treatment showed reduced size of right psoas abscess to 1.0×2.3×1.5 cm and disappeared left psoas abscess (Fig. 2). A repeated blood culture performed on 14 days and 30 days after admission revealed no growth. After 30 days of intravenous antibiotic therapy, he was discharged with oral cefixime for 2 weeks. He was afebrile on control visit in outpatient clinic after 2 weeks.
DISCUSSION
A ureae is a small, non-motile, vacuolated, bipolarstaining, pleomorphic organism and is gram-negative rod that grows well on media containing blood. The organism is most often a harmless commensal. However, under conditions of immune compromise or disruption of normal physical barriers to infection, it can lead to serious illness. Various predisposing condition such as postsurgical infection, periodontal disease, emphysema, alcohol related cirrhosis, skull fracture, alcohol abuse, neurosurgery, schizophrenia, odontal infection, diabetes, HIV infection/AIDS, Waldenstrom macroglobulinemia, COPD, malnutrition, rheumatoid arthritis, HCV hepatitis, etanercept, or methotrexate have been associated with infections caused by A. ureae (1-15). In this case, chronic hepatitis B was an underlying immune-compromised condition, which is a predisposing factor that is not previously mentioned in literature, and this may impair the defense against the organism. As most of the genus Actinobacillus species are commensal or pathogens of animals, especially cattle, horses, and pigs, history of trauma or recreational activities may provide important clues for establishing early diagnosis (15, 16). This patient had a history of slip-down injury while working at his farm. Therefore, it could be postulated that the origin of A.ureae in this case is from environmental localized mammalian flora.
Since its first description by Minter in 1881 (17), a psoas abscess has been a rare, but life threatening disea.se. The psoas muscle lies in close proximity to organs such as the sigmoid colon, appendix, jejunum, ureters, abdominal aorta, kidneys, pancreas, spine, and iliac lymph nodes. Hence infection in these organs can spread to the iliopsoas muscle. The abundant blood supply of psoas muscle is believed to be a predisposing factor for hematogenous spread from occult sites of infection (18) and this is called primary psoas abscess. About 18-20% of primary psoas abscess is associated with history of trauma (19). Thus this case could also be classified as primary psoas abscess. Staphylococcus aureus is the most common causative organism of primary psoas abscess and Streptococcus species and Escherichia coli are common in secondary psoas abscess (19).
A.ureae strains are susceptible to most antimicrobials including ampicillin, cephalothin, cefoxitin, tetracycline, aminoglycosides, and trimethoprim-sulfamethoxazole. Penicillin is favored as the first line antibiotic for invasive disease, followed by erythromycin and third-generation cephalosporins (15). In this case, the isolate showed susceptibility to all antibiotics and he was successfully treated with ceftazidime.
Other diagnostic modalities are available. Molecular biology-based techniques have proved useful for the detection and identification of organisms that are difficult or impossible to culture in vitro. In addition, analysis of DNA sequences has been used to name organisms that were unidentifiable by phenotypic testing (20).
Of the documented cases in the literature, this is the first case, to our knowledge, of a serious A.ureae infection associated with psoas muscle abscess that has been documented in HBV carrier without progression to liver cirrhosis. When a patient with psoas muscle abscess is found, the possibility that uncommon organism could be the cause of infection should always be seriously considered and effort should be made to identify species and obtain antibiotic susceptibility. This will lead to early initiation of appropriate antibiotic therapy resulting in successful treatment outcome.


 XML Download
XML Download