

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Q fever is a zoonosis caused by Coxiella burnetii, presenting as acute and chronic illness and it has been reported worldwide. Acute Q fever is usually asymptomatic or mild and self-limiting, but infective endocarditis is one of the most serious complications of chronic Q fever and can be fatal. Known risk factors for Q fever endocarditis are valvular heart disease, immunocompromised hosts, and pregnancy. There have been some reports on Q fever in Korea but there exists no report on Q fever endocarditis. We have experienced 2 cases of Q fever with underlying valvular heart disease; both patients came to the hospital for evaluation of prolonged fever. Although Q fever and Q fever endocarditis are rare in Korea, Q fever endocarditis should be considered in the differential diagnosis of patient with infective endocarditis when causative microorganism cannot be identified.
Figures and Tables
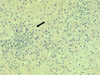 | Fig. 2Liver biopsy of case-1 shows multifocal lymphocyte infiltration, moderate inflammation, and multifocal spotty hepatic necrosis (H & E stain, ×200).
|
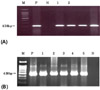 | Fig. 3PCR for C. burnetii. A) Case-1 : 1-blood sample on May 3, 2007, 2-blood sample on May 22, 2008 and case 2, B) Case-2 : 1 and 2-blood sample on Jan. 22, 2008, 3-blood sample on Nov. 26, 2008, 4-blood sample on Dec. 3, 2008, 5-tissue from valve surgery. M: marker, P: positive control with DNA for C. burnetii, N: negative control.
|

References
1. Maurin M, Raoult D. Q fever. Clin Microbiol Rev. 1999. 12:518–553.

2. Shin YJ, Yoo NC, Choi W, Yang DG, Lee HL, Cheon SH, Chang J, Kim SK, Lee WY. A case of Q fever. Korean J Med. 1992. 42:690–698.
3. Heo ST, Park MY, Choi YS, Oh WS, Ko KS, Peck KR, Song JH. Q fever as a cause of fever of unknown origin. Korean J Med. 2008. 74:100–105.
4. An SJ, Koo JW, Chung CY, Lee WY. A case of Q fever: person-to-person transmission. J Korean Pediatr Soc. 1998. 41:120–124.
5. Kim KS, Lee WY. Coxiella burnetii infection in patients with various diseases. J Korean Pediatr Soc. 1994. 37:356–367.
6. Park HS, Lee EG, Lee SY, Lyu CJ, Son YM, Kim DS, Kim KY, Lee WY. A case of Q fever: associated with pancytopenia, hepatitis, and myocarditis. Korean J Infect Dis. 1992. 24:45–54.
7. Park MS, Park MY, Shin YO. Distribution of antibidies to Coxiella burnetii in patients with unknown fever and atypical pneumonia. J Bacteriol Virol. 2003. 33:307–315.
8. Tissot-Dupont H, Raoult D. Q Fever. Infect Dis Clin North Am. 2008. 22:505–514.
9. Raoult D, Marrie T, Mege J. Natural history and pathophysiology of Q fever. Lancet Infect Dis. 2005. 5:219–226.
10. Hartzell JD, Wood-Morris RN, Martinez LJ, Trotta RF. Q fever: epidemiology, diagnosis, and treatment. Mayo Clin Proc. 2008. 83:574–579.
11. Kim WJ, Hahn TW, Kim DY, Lee MG, Jung KS, Ogawa M, Kishimoto T, Lee ME, Lee SJ. Seroprevalence of Coxiella burnetii infection in dairy cattle and non-symptomatic people for routine health screening in Korea. J Korean Med Sci. 2006. 21:823–826.
12. Calza L, Attard L, Manfredi R, Chiodo F. Doxycycline and chloroquine as treatment for chronic Q fever endocarditis. J Infect. 2002. 45:127–129.
13. Raoult D, Houpikian P, Tissot Dupont H, Riss JM, Arditi-Djiane J, Brouqui P. Treatment of Q fever endocarditis: comparison of 2 regimens containing doxycycline and ofloxacin or hydroxychloroquine. Arch Intern Med. 1999. 159:167–173.
14. Botelho-Nevers E, Fournier PE, Richet H, Fenollar F, Lepidi H, Foucault C, Branchereau A, Piquet P, Maurin M, Raoult D. Coxiella burnetii infection of aortic aneurysms or vascular grafts: report of 30 new cases and evaluation of outcome. Eur J Clin Microbiol Infect Dis. 2007. 26:635–640.
15. Fournier PE, Casalta JP, Piquet P, Tournigand P, Branchereau A, Raoult D. Coxiella burnetii infection of aneurysms or vascular grafts: report of seven cases and review. Clin Infect Dis. 1998. 26:116–121.
 XML Download
XML Download