

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Yellow fever (YF) is a viral hemorrhagic fever transmitted by daytime-biting mosquitoes lurking in sub-Saharan Africa and South America (1). Its clinical spectrum ranges from subclinical infection to an overwhelming systemic disease in approximately 15 to 20% of the infected persons, and its overall fatality rate is about 20 to 50% in some outbreaks. Since there is no specific therapy for YF and the treatment is supportive vaccination is very important (2). Thus, the YF endemic countries legally require travelers to submit an international certificate of vaccination from WHO-approved centers (3, 4).
The currently available vaccines are attenuated live virus vaccines derived from a virus originally isolated in 1927 and protect against all YF virus strains. They have been effective for several decades now, effectively protecting the vaccinees probably for a lifetime after the administration of a single dose (5, 6). The YF-vaccine-associated adverse events are generally mild, but the vaccine may cause serious problems in a small proportion of vaccinees (7, 8).
Due to the recent increase in international travel, many people are taking the YF vaccine, but studies on the adverse events of the YF vaccine are rare in Korea. This prospective study was thus conducted to evaluate the adverse events following YF vaccination on the Koreans.
Materials and Methods
1. Study design
Among the travelers who visited the International Travelers' Clinic of National Medical Center (NMC) for YF vaccination from January to December 2007, 318 gave documented consent to participate in this study. Individuals younger than nine months of age, and all the subjects with contraindications to YF vaccination, such as an immunocompromised condition and hypersensitivity to eggs or egg products were excluded from the study. The following data were collected prior to the vaccination: the subjects' age, sex, allergy history, presence of chronic illness, destinations, travel purposes, duration of their stay in the YF endemic zone, and occupations. Data or information regarding the adverse events of the vaccination were collected through six telephone interviews on days 3, 6, 9, 16, 23, and 30, after the immunization. The medical doctors who were fully informed of YF vaccine gathered the data by using a type of open-ended question about adverse events and afterwards sorted out the symptoms due to other medical problems through history taking. The adverse events were classified into 3 categories according to the severity: mild, moderate, severe. In the mild group, symptoms were perceived but there were no influences on regular activity and subsided spontaneously within 5 days; in the moderate group, the symptoms lasted more than 5 days or interfered with normal activity; in the severe group, the symptoms were severe enough to oblige the vaccinees to visit a health care center for medical intervention.
Nine (2.8%) participants who failed to complete the six telephone interviews were excluded from the analysis. Finally, 309 (97.2%) subjects were prospectively enrolled for the evaluation of the adverse event of the YF vaccination on them. All the subjects were immunized with the 17DD strain vaccine (Bio-Manguinhos, Rio de Janeiro, Brazil).
RESULTS
1. Characteristics of the subjects
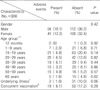
The 309 subjects, of whom 168 (54.4%) were males, were aged 11 months to 70 years, and their median age was 26.0 years (IQR: 15.0-41.0). The subjects were classified by their age group as shown in table 1. The peak vaccination incidence was highest in the age 10 to 19-year-old group which was 27.2%. Twenty (6.4%) recipients were over 60 years old, and 1 (0.3%) infant was less than 1 year old.
In this study, 34 (11.0%) subjects had underlying illnesses (Table 1). Concurrent immunization, such as with the influenza vaccine, oral typhoid fever vaccine, hepatitis A vaccine, hepatitis B vaccine, tetanus toxoid-diphteria toxoid vaccine, and antimalarial drugs, were documented in 72 (23.3%) cases. Of all the subjects, 237 (76.7%) subjects were only vaccinated with the YF vaccine, and one had received a prior YF shot.
2. Postvaccinal Adverse events
A total of 106 adverse events were noted in 97 (31.1%) subjects. The common systemic symptoms were headache (14.1%), mild fever (13.4%), and fatigue (11.3%), with local events occurring on the injected site (36.1%) (Table 2). These events were observed in 64 (66.0%) subjects within the first three days, in 30 (30.9%) subjects on days 4 through 9, and in 3 (3.1%) subjects after day 10. Most of the adverse events subsided within 3 to 4 days (Fig. 1). Both the systemic and local events were self-limiting and didn't interfere with normal activity.
In the group aged 10 to 19 years, the adverse events occurred more frequently (32%), but the frequency of their occurrence was not statistically significant (P=0.14). Five (1.6%) subjects aged over 60 years suffered from adverse events, its frequency was statistically insignificant (P=0.62).
Three subjects with underlying illnesses (1.0%) experienced adverse events; the subjects were suffering from hypertension (P=0.64), allergic rhinitis (P=0.32), or atherosclerosis (P=0.08).
Among those who were concurrently immunized with other vaccines, adverse events occurred in 19 travelers (6.1%); 15 subjects out of 56 persons who had an additional vaccination, 2 subjects out of 8 persons who had two additional vaccinations, and 1 subject out of 3 persons who had four additional vaccinations experienced adverse events but concurrent immunization did not increase the risk of the occurrence of adverse events with their p values being 0.41, 0.71, and 0.67, respectively.
Discussion
The YF vaccine virus is grown in chicken embryos that had been inoculated with a seed virus of a fixed passage level. Two substrains were independently derived from 17D: 17DD and 17D-204. These two substrains share a 99.9% sequence homology, and both lead to a 98% seroconversion among healthy adults (9, 10). It is estimated that over 500 million doses of the vaccine have been used, with an excellent safety record. Approximately 1% of the vaccinees had severe adverse events. The previous reports showed that the risk factors of considerable adverse events after the administration of the vaccine appeared in the following groups: infants younger than 9 months old, the elderly, immunosuppressed patients, subjects with underlying diseases, individuals with hypersensitivity to eggs or egg products, and those with thymus disease (11, 12).
Infants younger than 6 months old and adults over 60 years old are more susceptible to the serious adverse events due to YF vaccination. This age-related risk was found to be more pronounced for YF-vaccine-associated viscerotropic and neurotropic diseases, although the incidences are very rare. Postvaccinal encephalitis occurs principally in very young infants, and viscerotropic events develop mainly in persons relatively advanced in age (2, 6, 13). An increased risk of acquiring severe adverse events due to YF vaccine virus among the older recipients of the vaccine is biologically plausible. In one research conducted in the U.S., the reporting rate for systemic illnesses requiring hospitalization or leading to death after YF vaccination was 8.3 per 100,000 doses for those over 65 years of age, and 18.1 per 100,000 doses for those over 75 years of age (14, 15).
In this study, the adverse events of YF vaccination could not be evaluated in infants younger than 9 months old, in immunosuppressed patients, individuals with hypersensitivity to eggs or egg products, and who had had a thymus disease, as they were excluded from the study. The adverse events of YF vaccination in the group aged over 60 years did not occur frequently in this study (P=0.62), which differs from the results of the previous studies (16). This might actually prove that there's little difference in response to YF vaccine according to age distribution in Korean population. However, it is also possible that the population selected in this study has been biased thus not fully representing the group mostly affected or the so-called "healthy vaccine effect" might have occurred in which, the subjects are very healthy and immunologically competent that they are less prone to suffer from adverse events.
The incidence of adverse events due to YF vaccination in the group aged 10 to 19 years in this study was higher than in the other groups, although the frequency had no statistical significance. This may be attributed to the fact that the subjects in this age group might have been more willing to report their symptoms, and that the groups that were vulnerable to the adverse events of YF vaccination have been excluded from the study.
The subjects with underlying illnesses complained more frequently of adverse events of YF vaccination (3 out of 34 persons), but their number was not statistically significant and there was no evidence of aggravation of the illnesses.
With the increase in the number of long-standing and adventurous travelers, the importance of concurrent immunization with "travel vaccines" is increasing because the countries in which YF is endemic often bear the brunt of several waves of concomitant epidemics, such as malaria, typhoid fever, poliomyelitis, and measles (17, 18). In this study, 72 (23.3%) subjects were given other vaccines simultaneously with the YF vaccine. Among them, 19 (6.1%) recipients reported adverse events, which consisted of 20 (6.5%) systemic and eight (2.6%) local symptoms. No increased risk was found in relation to the numbers and types of other vaccines that had been administered to the subjects. Also, the incidence rates were much lower than those in the previous studies, in which 47% experienced local events and 22% developed systemic adverse events after the combined vaccination (19). However, enhanced surveillance is required to clarify the relationship regarding specific kinds or numbers of other vaccines.
Within the investigation period, no life-threatening adverse events were reported. This result seems to be related to the fact that high-risk individuals were not included in this study. And certain limitation in estimating the severity may exist because medical examination was done just by interviewing without recourse to any other methods.
In addition, 12 (3.9%) subjects who were younger than 4 years old, who might have had problems expressing the symptoms, were included in this study and their information regarding adverse event were provided by the parents. If the symptoms were unnoticeable, it might not have been perceived by the parents and might have been underestimated in these subjects. Therefore, in comparison with other subjects, who could report the symptom for themselves, the real incidence of adverse events in younger subjects may be higher than the result from this study.
To our knowledge, this research is the first major study ever conducted on the adverse events of the YF vaccine on the Korean population. In this study, postvaccinal adverse events were reported by 31.4% of the vaccinees, and all the reported symptoms were mild and self-limiting. Therefore, the Korean travelers to YF endemic zones can undergo YF vaccination without fear of serious adverse events if they do not have any contraindication to the vaccine.


 XML Download
XML Download