

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Syphilis caused by the spirochete Treponema pallidum is a reemerging disease that is sexually transmitted and can progress in stages (1). As culture of T. pallidumis not possible, diagnosis of syphilis in many cases depends on serologic methods.
Since the rapid plasma reagin (RPR) card test is easy to use, inexpensive, and its sensitivity and specificity are equal to or better than those of the VDRL test, it is widely used as a screening test for syphilis (2). The sensitivity of the non-treponemal tests depends on the stage of syphilis (3, 4). The sensitivity of RPR test inthe primary, secondary, latent, and late stages is 86%, 100%, 98%, and 73%, respectively, according to the centers for disease control and prevention (CDC) studies (5).
Recently developed quantitative automated RPR latex turbidimetric immunoagglutination (LTIA) test is different from RPR card test in two aspects. First, RPR LTIA test is performed with routine chemistry equipment compared to RPR card test which is performed manually. Second, interpretation of the test result is made by means of immunologic reaction and has good reproducibility, whereas RPR card test is read with the naked eye, which can affect the result of the test depending on the skillfulness of technicians (6). When everything is considered, the sensitivity and specificity of test results and the significance of the diagnostic findings depend primarily on the expertise of the individual laboratory and the test manufacturer (1).
Irrespective of the automated quantitative RPR test being gradually set-up, clinical consensus on this new test is still not well established in South Korea. The purpose of this study was to evaluate the validity of quantitative RPR LTIA, HiSens Auto RPR LTIA (HBi Corp., South Korea) and to decide an adequate cutoff value for syphilis screening.
Materials and Methods
From January 2007 to July 2007, a total of 549 serums or plasma specimens from patients were tested with HiSens Auto RPR LTIA (HBi Corp) and Asan RPR card test (Asan RPR card test, Asan Pharm Corp., Hwaseong, Gyeonggi, South Korea). HiSens Auto RPR LTIA is a latex turbidimetric immunoagglutination test using cardiolipin and lecithin antigen to detect syphilis antibody in patient's serum. It is reported as positive when its value is above 2.5 R.U., and measurable range is up to 20 R.U. The cases in which RPR card test was positive, T. pallidum hemagglutination (TPHA) (Asan-TPHA, Asan Pharm Corp., Hwaseong, Gyeonggi, South Korea) was tested to confirm syphilis. RPR LTIA was tested with the chemistry analyzer, ADVIA 2400 (Bayer Corp., Tarrytown, NY10591-5097, USA).
The authors arbitrarily divided cutoff values from 2.5, set by the manufacturer, into nine values with 0.3 intervals (cutoff values of 0.1, 0.4, 0.7, 1.0, 1.3, 1.6, 1.9, 2.2, and 2.5). Four categories were made according to the test results of RPR card and RPR LTIA: Card (+)/LTIA (+), Card (+)/LTIA (-), Card (-)/ LTIA (+), and Card (-)/LTIA (-). The degree of agreement between RPR card test and RPR LTIA test was analyzed at given cutoff values of RPR LTIA test. Kappa value was calculated according to the equation, k=(OP-EP)/(1-EP), where OP is the observed proportion of agreement between the two tests, and EP is the expected proportion of agreement due to chance (7). Kappa value was interpreted as follows: <0, no agreement; 0.0-0.20, slight agreement; 0.21-0.40, fair agreement; 0.41-0.60, moderate agreement; 0.61-0.8, substantial agreement; 0.81-1.00, almost perfect agreement (8).
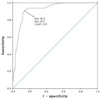
Patients were divided into two groups according to the results of RPR card and TPHA tests: 1) a syphilis test positive group (RPR card positive and TPHA positive group, N=66), 2) a syphilis test negative group (RPR card negative and TPHA negative group, N=452). To test validity of a RPR LTIA test, the area under the ROC curve (AUC) was measured in this setting. AUC ranges between 1.0 (perfect separation of the test values of the two groups) and 0.5 (no apparent distributional differences between the two groups of test values) (9, 10). The closer the value approached 1.0 and the ROC curve moved towards the left and top boundaries of the ROC graph, the more we considered it had apparent distributional difference between the two groups of test values.
The analyses for ROC curve, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of RPR LTIA test were performed to decide a cutoff value of RPR LTIA test at desirable sensitivity and specificity in this setting.
Additionally, distributions of the test results showing disagreement between RPR card test and RPR LTIA test were analyzed. T. pallidum antibody (TPAb, HiSens auto TP LTIA, HBi Corp) test was performed together with TPHA test in 82 specimens for the degree of agreement between these tests.
Statistical analysis was carried out using SPSS for Windows statistics program (version 13, SPSS Inc, Chicago, USA). A P value of less than 0.05 was considered statistically significant.
Results
In degree of agreement analysis, numbers of cases at given cutoff values were distributed between 36- 80, 0-44, 15-347, and 122-454 in Card (+)/LTIA (+), Card (+)/LTIA (-), Card (-)/LTIA (+), and Card (-)/LTIA (-), respectively (Table 1). Agreement analysis showed slight to moderate agreement depending on the given cutoff values (k=0.093-0.588, P=0.000) (Table 1). Kappa value had its highest value at the cutoff value of 1.3 and 1.6 (k=0.588, P=0.000). Kappa value at the cutoff value of 1 ranked second (k=0.578. P=0.000).
A plot of ROC curve showed a statistically valid result regarding the differentiation between a syphilis test positive group and a syphilis test negative group with RPR LTIA test (AUC=0.92, P=0.000) (Fig. 1).
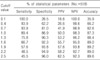
The cutoff value in RPR LTIA test ranged between 0.65 and 1.15 when both sensitivities and specificities were higher than 80%. Sensitivity and specificity at cutoff values of 0.1, 0.4, 0.7, 1.0, 1.3, 1.6, 1.9, 2.2, and 2.5 were distributed from 45.5% to 100% and from 26.5% to 96%, respectively (Table 2). PPVs at those cutoff values were distributed from 16.6% to 62.5% and NPVs were excellent at all cutoff values (92.3-100%) (Table 2).
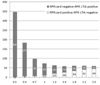
Although the number of discordant test results was increased at the cutoff value of 1.9, 2.2 to 2.5 (60, 61, and 59, respectively), the number of discordant tests at other cutoff values (from 0.1 to 1.6) were decreased with increasing cutoff values (Fig. 2).
Kappa analysis showed almost perfect agreement between TPAb test and TPHA test (k=0.826, P=0.000) (Table 3).
Discussion
The clinical relevance of the results obtained in a test to diagnose syphilis, the simplicity with which the test can be performed, and the test's sensitivity and specificity must be considered before a new test is placed into routine use in the clinical laboratory (5). RPR card test is widely used as a screening test for syphilis in South Korea with confirmatory test being TPHA or fluorescent treponemal antibody absorption assay (FTA-ABS). Screening test and confirmatory test are not tested at the same time in most cases because of restrictive medical insurance system in South Korea and cost-effectiveness. Clinicians usually use RPR card test for screening syphilis in patients who are to undergo surgery, suspected to have syphilis or having a routine medical examination. Since the routinely performed RPR card test is thought to be laborious and the result could be affected by technicians' skill and point of view, there is a general consensus that a novel method that is more reproducible, convenient, and automated is needed.
As for the agreement between RPR card test and RPR LTIA test, the kappa value (k) at the cutoff level of 1.3 or 1.6 showed the best result among other cutoff values. However, the sensitivities at those cutoff values were lower than that at the cutoff value of 1 (66.7%, 75.8% and 89.4% at the cutoff value of 1.6, 1.3, and 1.0, respectively). Considering the generally accepted sensitivity of syphilis testing, simply setting a cutoff value according to the results of agreement analysis is not appropriate. As described in table 2, the accuracy at the cutoff value of 2.5 is first-ranked. However, in table 1, the k statistic showed lower k value even when compared to the cutoff value of 1.9 which was second-ranked. Accuracy is calculated by the formula of (true positive + true negative) / (true positive + false positive + false negative + true negative). k is a ratio of the observed improvement over chance agreement to the maximum possible improvement over chance (7). Hence, the chances of clinicians being confused would increase at the cutoff value of 2.5 due to the increased disagreement irrespective of its high accuracy. Furthermore, low sensitivity at this cutoff value (45.5%) cannot be admitted as a screening test. As syphilis is a quite rare but serious disease, the importance of routine screening test for syphilis cannot be overlooked. Furthermore, screening for syphilis places a premium on sensitivity rather than on specificity because syphilis can be effectively treated and additional cost is high when it is left alone.
Area under the ROC curve (0.92), good sensitivity and specificity at the cutoff value of 1 (89.4%, and 86.9% respectively), and automated procedure combine to create a positive perception of the test. However, if RPR LTIA is set to have sensitivity similar to that of the RPR card test, the PPV decreases compared to that of the RPR card test, which might cause clinicians some confusion. To keep up with the similar sensitivity, clinicians have to accept a relatively high false positive rate. In contrast to the past, clinicians may more often have to order a TPHA or FTA-ABS test for confirmation.
At the cutoff value of 1, the sensitivity is 89.4% but the PPV is as low as 50%. However, at the cutoff value of 2.5, the sensitivity and PPV were 45.5% and 62.5%, respectively. This phenomenon is true to all cutoff values. As PPV is calculated as the number of true-positives/(true positives + false positives), false positive portion could increased in cases of high sensitivity and low PPV. When the cutoff value is set at a high PPV and low sensitivity, many probable syphilis patients could be lost at the screening phase. The prevalence of a disease in a population also affects screening test performance; in low-prevalence settings, even very good tests have poor positive predictive values (11). With regard to reactivity in VDRL and RPR card testing, more than 20% of VDRL positive patients and about 10% of RPR card test positive patients of study population were reported as biologic false positive (12-16).
As cutoff values were decreased to increase sensitivity, many patients who were negative with RPR card test became positive with RPR LTIA test; 62 patients negative with RPR card test became positive with RPR LTIA test at the cutoff value of 1, which might increase false positive portion. Conversely, many patients who were positive with RPR card test appeared to be negative with RPR LTIA test at high cutoff values 44 patients positive with RPR card test became negative with RPR LTIA test at the cutoff value of 2.5. This means probable syphilis patients could be missed at the cutoff value of 2.5.
In practical use of RPR LTIA test, an adjuvant test algorithm should be devised to compensate for expected demerits especially related to false positive results. As a good supplementary test for the RPR LTIA test system, TPAb test is thought to be very feasible. TPAb is a treponemal test for syphilis and the correlation between TPAb and TPHA was excellent when evaluated (k=0.826, P=0.000, Table 3). It can also be tested in automated routine chemistry analyzers. When the test results of RPR LTIA have values higher than the cutoff level, TPAb can automatically be ordered to be tested in the same chemistry equipment using a programmed algorithm set in advance. Well-designed test algorithm for syphilis is expected to remove both unexpected false positive and false negative results and increase the accuracy of syphilis diagnosis.
Although it seems somewhat worrying to use the RPR LTIA test alone without supporting devices like the previously-mentioned test algorithm, to screen syphilis in huge numberof patients effectively and accurately, an automated quantitative test kit will be an indispensable tool. So, it is believed that we should make a supportive plan for this new test,at least until a more refined and accurate quantitative screening test method for syphilis is established. Strictly speaking, this new quantitative method still seems to have problems in practical use. Nevertheless, many hospitals in Korea have already set up such tests using latex immunoagglutination methods (17). There may be several causes related to this. First, laboratory medicine doctors want both fast and accurate automated manipulation for the effective management of laboratory practice. Second, syphilis is not considered as serious a disease as cancer or other life-threatening conditions. The RPR test is performed to screen a population consisting of a majority of uninfected people and a minority of infected patients. As a result, laboratory medicine doctors may not perceive the potential problems as serious.
In conclusion, considering the importance of sensitivity in screening for syphilis and the degree of agreement with RPR card test, the cutoff value of 1 in HiSens Auto RPR LTIA test is thought to be adequate. To minimize the probable false positive portion, a supportive test algorithm including an additional test with high specificity is recommended when the test results of RPR LTIA test are higher than the value set as the cutoff-value. Additionally, further evaluation on the correlation between the titer of the RPR card test and quantitation of RPR LTIA should be considered to be able to completely substitute the RPR card test, the widely-used test for syphilis screening.


 XML Download
XML Download