

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ho Young Lee, M.D.1, Tae Hyong Kim, M.D.1 , Eun Ju Choo, M.D.1, Min Hyok Jeon, M.D.1, Eun Jeung Lee, M.D.1, Eun Jung Jung, M.D.1, Seong Ran Jeon, M.D.1, Eui Ju Park, M.D.1, Wook Youm, M.D.2, Won Ho Jang, M.D.2, Jeong-Hwa Hwang, M.D.3, Dong Hun Kim, M.D.3, Dong Won Kim, M.D.4
, Eun Ju Choo, M.D.1, Min Hyok Jeon, M.D.1, Eun Jeung Lee, M.D.1, Eun Jung Jung, M.D.1, Seong Ran Jeon, M.D.1, Eui Ju Park, M.D.1, Wook Youm, M.D.2, Won Ho Jang, M.D.2, Jeong-Hwa Hwang, M.D.3, Dong Hun Kim, M.D.3, Dong Won Kim, M.D.4
, Eun Ju Choo, M.D.1, Min Hyok Jeon, M.D.1, Eun Jeung Lee, M.D.1, Eun Jung Jung, M.D.1, Seong Ran Jeon, M.D.1, Eui Ju Park, M.D.1, Wook Youm, M.D.2, Won Ho Jang, M.D.2, Jeong-Hwa Hwang, M.D.3, Dong Hun Kim, M.D.3, Dong Won Kim, M.D.4
Abstract
Infected aneurysms are uncommon, frequently fatal lesions. "True" fungus-infected aneurysms are even rarer. Fungal infections have high morbidity and mortality. However, diagnosis is frequently difficult, since the symptoms are non-specific and standard diagnostic procedures are often insensitive. We experienced a patient with persistent fever and negative blood cultures. The patient was immunocompetent and had no risk factors, and was diagnosed with a fungus-infected aneurysm based on computed tomography and vascular surgery. The vascular tissue revealed some narrow-based budding yeast within the thrombus, suggesting Candida infection. Seventeen cases of infected aneurysm of the abdomen were reported in Korea from 1988 to 2007, although none were "true" fungus-infected aneurysms, making this the first fungus-infected aneurysm of the abdomen in Korea. Prompt diagnostic procedures and aggressive treatment modalities are necessary for patients with occult infection and negative blood cultures, regardless of their immunocompetence, because of the high morbidity and mortality of this condition.
Figures and Tables
Fig. 1
Microscopic findings of the aneurysm with a thrombus (arrow). (A) (H & E, ×12.5) and marked infiltration of lymphocytes, plasma cells, and histiocytes in the wall (B) (H & E, ×400). Microscopic findings of the thrombi, showing irregular and ill-defined laminations (C) (H & E, ×12.5) and partly necrotic tissue with acute and chronic inflammatory cells (D) (H & E, ×100). A few yeast are present within the thrombi (E) (GMS, ×100) and a narrow-based budding yeast (arrow) (F) (GMS, ×400).

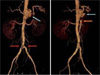
Fig. 2
Multidetector CT (MDCT) demonstration of thrombosed abdominal aortic aneurysms in a patient with infectious aortitis. A, B : Coronal MDCT images demonstrate aneurysmal dilatation of proximal abdominal aorta (arrows in A) and also involvement of distal abdominal aorta extending to aortic bifurcation and proximal both common iliac arteries (arrows in B).

Fig. 3
Axial MDCT images demonstrate aneurysmal dilatation of proximal abdominal aorta associated with irregular circumferential thrombus and periaortic enhancement consistent with active mural disease (arrows in A). Extension of inflammation into aortic branch vessels is well shown surrounding origin of the celiac artery (arrows in B) and superior mesenteric artery (arrows in C).

Fig. 4
Axial MDCT images demonstrate separate involvement in distal abdominal aorta (A). MDCT images shows propagation of aortitis with thrombus into aortic bifurcation (arrows in B) and proximal both common iliac arteries (arrows in C).

Fig. 5
MDCT with volume rendering (VR) reformation images nicely demonstrate proximal abdominal aortic aneurysm (blue arrow in A) and irregular luminal narrowing in distal abdominal aorta and proximal both common iliac arteries (red arrows in A). Origination of the celiac artery (blue arrow in B) and superior mesenteric artery (red arrow in B) from the dilated proximal abdominal aorta is well shown on right oblique sagittal VR image.

References
1. Parkhurst GF, Dekcer JP. Bacterial aortitis and mycotic aneurysm of the aorta; a report of twelve cases. Am J Pathol. 1955. 31:821–835.
2. Oderich GS, Panneton JM, Bower TC, Cherry KJ, Rowland CM, Noel AA, Hallett JW, Gloviczki P. Infected aortic aneurysms: Aggressive presentation, complicated early outcome, but durable results. J Vasc Surg. 2001. 34:900–908.

3. Ewart JM, Burke ML, Bunt TJ. Spontaneous abdominal aortic infections. Essentials of diagnosis and management. Am Surg. 1983. 49:37–50.
4. Potti A, Danielson B, Sen K. "True" mycotic aneurysm of a renal artery allograft. Am J Kidney Dis. 1998. 31:E3.
5. Werner K, Tarasoutchi F, Lunardi W, Mariño JC, Grinberg M, Bellotti G, Jatene AD. Mycotic aneurysm of the celiac trunk and superior mesenteric artery in a case of infective endocarditis. J Cardiovasc Surg (Torino). 1991. 32:380–383.
6. Gauto AR, Cone LA, Woodard DR, Mahler RJ, Lynch RD, Stoltzman DH. Arterial infections due to Listeria monocytogenes: report of four cases and review of world literature. Clin Infect Dis. 1992. 14:23–28.
7. Walsh TJ, Hutchins GM. Aspergillus mural endocarditis. Am J Clin Pathol. 1979. 71:640–644.
8. Manuel RJ, Kibbler CC. The epidemiology and prevention of invasive aspergillosis. J Hosp Infect. 1998. 39:95–109.
9. Sanchez-Recalde A, Maté I, Merino JL, Simon RS, Sobrino JA. Aspergillus aortitis after cardiac surgery. J Am Coll Cardiol. 2003. 41:152–156.
10. Fisher JF, Chew WH, Shadomy S, Duma RJ, Mayhall CG, House WC. Urinary tract infections due to Candida albicans. Rev Infect Dis. 1982. 4:1107–1118.
11. Davutoglu V, Soydinc S, Aydin A, Karakok M. Rapidly advancing invasive endomyocardial aspergillosis. J Am Soc Echocardiogr. 2005. 18:185–187.
12. Gonda RL Jr, Gutierrez OH, Azodo MV. Mycotic aneurysms of the aorta: radiologic features. Radiology. 1988. 168:343–346.
13. Ljungman P, von Döbeln L, Ringholm L, Lewensohn-Fuchs I, Klingspor L, Sparrelid E. The value of CMV and fungal PCR for monitoring for acute leukaemia and autologous stem cell transplant patients. Scand J Infect Dis. 2005. 37:121–127.
14. Chung JW, Park SJ, Sung H, Kim MN, Kim BS, Lee SG. A Case of Disseminated Infection Due to Scedosporium apiospermum in a Liver-transplantation Recipient. Korean J Lab Med. 2005. 25:421–424.
15. Rutherford RB. Vascular surgery. 1989. 3rd ed. Philadelphia: WB Saunders;969.
 XML Download
XML Download