

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Human cytomegalovirus (HCMV) is a common human pathogen that causes morbidity and mortality in hematopoietic stem cell transplantation (HSCT) recipients (1-3). Early diagnosis of HCMV infection or reactivation and effective pre-emptive therapies with setting cut-off values are required for appropriate HCMV disease prevention in HSCT recipients (4-6) Although the antigenemia assay is one of the most widely used methods to monitor CMV infection or reactivation, this assay has many limitations: it requires high-level skill in the experimenter; it is very labor intensive and the specimens must be handled quickly (1, 3, 6-8). Recent reports suggest that HCMV infections with real-time PCR methods can be predicted more rapidly and sensitively than with the HCMV pp65 antigenemia assay (1, 7). Therefore, we compared the pp65 antigenemia assay and two kinds of quantitative HCMV real-time PCR methods in 67 patients who had undergone HSCT to apply the prediction of HCMV infections and reactivation.
Sixty-seven HSCT patients who had visited at a Korea Catholic Hematopoietic Stem Cell Transplantation Center between May 2000 and March 2002 were participated for this study. These patients were included in the study and gave their informed consent. There were 43 men and 24 women with the median age of 32 years (15-51 years). The median follow-up duration after organ transplant was 690 days (32-1,226 days) and the number of samples obtained from the 67 HSCT patients was 254. HCMV DNA was extracted from the plasma (0.2 mL) of HSCT recipients with a QIAamp Blood Mini Kit (Qiagen, Valencia, CA, USA) according to the manufacturer's instructions and the detection of HCMV DNA was determined by two distinct real-time PCR methods: Light Cycler-based PCR (LC PCR) and in-house immediate early protein-based PCR (in-house IE PCR). HCMV LC PCR was carried out using the commercial artus® CMV LC PCR kit (Qiagen, Hilden, Germany) and in-house IE PCR method was performed with the primers and probe reported by Ikewaki et al (7) The results for pp65 antigenemia assay were presented as the number of pp65-positive cells per 2 × 105 leukocytes (8).
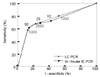
HCMV infection from 254 plasma samples was detected in 82 (32.3%) by pp65 antigenemia assay, in 112 (44.1%) by in-house IE PCR, and in 170 (66.9%) by LC PCR. The sensitivity and specificity of the two distinct real-time PCR methods based on the results of pp65 antigenemia assay were 82.9% and 40.7% in the LC PCR and 79.3% and 72.9% in the in-house IE PCR, respectively (Table 1). The correlations between the HCMV viral load and pp65 antigenemia in HSCT patients were r=0.603 with in-house IE PCR and r=0.525 with LC PCR, respectively (P<0.0001, Fig. 1). The above results showed that in-house IE PCR was higher specificity than the LC PCR.
To set the optimal cut-off values of the HCMV DNA load by the two distinct real-time PCR methods for detection of HCMV infection and reactivation, the receiver operating characteristic (ROC) curves were constructed using the eighty-two pp65 antigenemia positive samples (Fig. 2). When cut-off values of HCMV DNA load in the in house IE PCR were set as 10, 25, and 50 copies/ mL, the sensitivity and specificity for detection of HCMV infection were 72.1% and 57.1% at 10 copies/mL; 69.1% and 71.4% at 25 copies/mL; 60.3% and 85.7% at 50 copies/mL, respectively. When cut-off values of HCMV DNA load in LC PCR were set as 1,000, 2,500, and 5,000 copies/mL, the sensitivity and specificity for detection of HCMV infection were 80.0% and 47.1% at 1,000 copies/mL; 67.7% and 76.5% at 2,500 copies/mL; 56.9% and 88.2% 5,000 copies/mL, respectively. From these data, the optimal cut-off values, 25 copies/mL for in-house IE PCR and 2,500 copies/mL for LC PCR, were applied to detect HCMV infection and reactivation for eighteen naive HSCT patients and these cut-off values were useful (data not shown). Some studies suggested that the cut-off values of HCMV viral loads for preemptive therapy might differ such as 200 copies/ml and ≥ 10,000 copies/mL depending on the kind of real-time PCR method and clinical samples (7, 8, 10, 11).
In conclusion, these results suggest that the optimal cut-off values of HCMV viral load for pre-emptive therapy in HSCT recipients should be differently considered by each individual method including detection protocols and specimen type as DNA sources (plasma or whole blood).


 XML Download
XML Download