

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Methicillin resistant Staphylococcus aureus (MRSA) is one of the major causes of human infections and has increased rapidly during the past few decades (1, 2). Most of them have been associated with hospital or healthcare (HA-MRSA). The incidence of methicillin resistance among nosocomial isolates of S. aureus is now higher than 60% in Korea (3). Moreover, recent reports have described an increasing incidence of community-associated MRSA (CA-MRSA) in patients who do not exhibit established risk factors for HA-MRSA and it has become a major concern worldwide (2, 4).
Some epidemiological studies have suggested that most of CA-MRSA strains had association with lack of multi-drug resistance, predominance of staphylococcal cassette chromosome mec element (SCCmec) IV and high prevalence of Panton-Valentine leukocidin (PVL) genes (2, 4). Although there still have been some disputes about the contribution of PVL in pathogenesis, PVL could be one of important virulence determinants associated with severe infection (5-8). So it is important to monitor the emergence of such strain in human associated MRSA infection
PVL+ CA-MRSA strains, associated with human infection, have rarely been reported in Korea (9, 10), although some PVL+ MRSA strains were frequently isolated from bovine milk (11, 12).
In this report, we present a case of extensive perianal abscess due to PVL+ CA-MRSA in Korea. We also discuss its molecular characteristics, in comparison with the previously reported PVL+ strains from the Far East including China, Japan, Korea, and Taiwan.
CASE REPORT
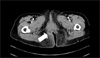
A 76-year-old woman presented with 2-week history of throbbing perianal pain that had worsened over preceding 2 days. Her medical history was notable for hypertension for 30 years but she had not been hospitalized in recent years nor received prolonged antibiotics or intravenous drugs. There was no known contact history with patients associated with S. aureus. However, she had a history of traveling to Hawaii for the last 2 weeks. Clinical examination revealed fever (39.3℃) and two circumferential huge perianal mass-like lesions. No cutaneous furuncle, carbuncle, or wound on the other site of skin was found. The initial laboratory test showed an elevated a white blood cell count of 19,380/mm3 (segment neutrophil 86%) and an increased C-reactive protein level of 40.45 mg/L (normal range, 0-5 mg/L). Computed tomography with contrast medium showed perianal inflammation, extending to the bilateral ischiorectal fascia, predominant in the right side (Figure 1).
Intravenous cefoperazone/sulbactam 1 g twice daily was started. After three days, incision and drainage was performed. From the cultures of blood on the first day and the drained pus on the third day grew pure growths of MRSA with same antibiogram (named strain of YSSA15). Antibiotic susceptibility test by disc diffusion according to the guidelines of the Clinical and Laboratory Standards Institute (2006) showed that the isolate was susceptible to gentamicin, clindamycin, fusidic acid, ciprofloxacin, tetracycline, trimethoprim/sulfamethoxazole and vancomycin (13). It was resistant only to penicillin, oxacillin, and erythromycin. Treatment was switched to vancomycin 1 g twice daily plus metronidazole 500 mg thrice daily for 1 week followed by 2 months of oral fusidic acid. Three months later after surgery, there was no clinical evidence of a residual abscess.
On the laboratory test, the presence of the mecA, nuc gene was confirmed by PCR, as described previously (14). To confirm the existence of PVL gene, we amplified its PVL genes (lukS-PV and lukF-PV) from YSSA15 for whole sequencing using the primers designated from GenBank No. AB006796 (forward lukS-PV; 5'-tgtttggtaatgaacgggttt-3', reverse lukS-PV; 5'-ggatagcaaaagcaatgcaa-3', forward lukF-PV; 5'-cacaacgcatttgtaaacagaaa-3', reverse lukF-PV; 5'-tcaattaagacgtggttaccctaa-3'), and cloned using pcr 2.1 TOPO kit (Invitrogen Corp., Calsbad, CA, USA). Then sequences after two sequencing data of PCR products (lukS-PV and lukF-PV) were assembled. The BLAST search (BLASTN 2.2.13) of assembled nucleotide sequencing result (GenBank No. DQ993352) showed over 99.5% of homology of USA300 (CP000255; 1546087-1548249). It was further analyzed to investigate other molecular features, including SCCmec, multilocus sequence typing (MLST), protein A gene (spa) typing, accessory gene regulator locus (agr) typing, hemolysin and staphylococcal enterotoxin genes, as previously described (2, 15). It was characterized as type IV SCCmec-ST8-type 1 spa-type I agr. Also it possessed alpha-, beta-, delta- and gamma-hemolysin variant. Among the staphylococcal enterotoxin genes, only sea was positive.
DISCUSSION
There have been several reports about molecular characteristics of MRSA isolated from Korea. ST5 or ST239 - SCCmec type II or III predominance were mainly presented in HA-MRSA. ST72 - SCCmec type IVA were predominant in CA-MRSA strains although CA-MRSA strains were still rare in Korea (9, 10, 12, 16-18). Strains of SCCmec type IV - ST8 from invasive disease like this report have not been reported in Korea yet.
From 2004 to 2005, we have collected of pathogenic MRSA strains for epidemiologic study from a university affiliated tertiary referral hospital and five community hospital in Seoul, Korea (16). Of total 81 strains of CA-MRSA by definition (1, 16), we found YSSA15 was the only one PVL+ isolate. And further molecular epidemiological findings revealed that this strain could be from internationally spread clone (USA300) (4). MRSA isolates with this genotype have recently been predominantly found in the United States, not in Japan and Taiwan (4, 19-23). The patient from our case had no history of frequent cutaneous infections or contact with patients suspicious of MRSA infection. However, the fact that the patient had been to Hawaii a few weeks ago before she suffered from MRSA infection made us to suspect that the organism might have been imported from Hawaii, USA. Also the possibility that MRSA came from bovine milk PVL+ clone in Korea was excluded, because their genetic background had no genetic relationship with YSSA15 (11). To validate whether this is the same isolate as USA300 reported previously, we are considering performing pulsed field gel electrophoresis with YSSA15 and USA300 from center for disease control and prevention in USA.
Clinical presentation of perianal abscess was unusually bilateral and extended to the regional fascia, these findings showed the possible role of PVL which is considered to contribute to the extensive progression of inflammation. Fortunately it was controlled by surgical drainage of appropriate timing and proper use of antibiotics. As CA-MRSA USA300 reported in the literature (24), YSSA15 was not multi-drug resistant, only resistant against penicillin, oxacillin, and erythromycin. In this case, β-lactams followed by vancomycin and oral fusidic acid were useful to control infection. However, it should be reserved for the use of other susceptible antibiotics such as quinoloes, clindamycin, etc. because of the risk of iMLSB resistance induction during treatment. And further studies are warranted.
We also reviewed the comprehensive literatures of PVL+ strains reported from the Far East (China, Japan, Taiwan) during 2000-2007 using a service of the National Library of Medicine and the National Institute of Health (http://www.ncib.nlm.nih.gov/entrez/query/fcgi?DB=pubmed) (19-22, 25) and compared their epidemiologic data, virulence and resistance characteristics with our isolate (Table 1). Even though they were not collected in the same manner, the prevalence of PVL gene tended to be much lower than in western countries (4) except in cases of Taiwan. In Japan, one PVL+ HA-MRSA strain was found to be associated with outbreaks in 1980-1990 (20). Additionally, diverse molecular types, hemolysin and enterotoxin genes were found as shown in Table 1. Antibiotic resistance patterns were also somewhat different according to countries. Although geographically close, it could be concluded that the genetic background of PVL+ strains were widely varied in the Far East.
It should be necessary to monitor the characteristics of CA-MRSA strains in Korea, although PVL positive strains are rare. It was revealed that the spectrum of epidemiology and virulence of PVL+ strain would be changed due to the adaptation with typical PVL-Japanese CA-MRSA strains (19). So these findings show us the importance of continuous surveillance strategy of the spreading of PVL+ pandemic strain and the changing pattern of major virulence factors in MRSA-associated disease. Moreover PVL gene could be horizontally transmitted to other strains via temperate bacteriophage (26).
In summary, we report a first case of perianal abscess due to PVL+ CA-MRSA strain in Korea which is homologous with USA300. In the literature review, PVL+ MRSA were not frequently found in the Far East except in Taiwan. Other molecular characteristics of strains were distinguishable from each other according to countries.

 XML Download
XML Download