

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Platelet P2Y12 receptor inhibitor non-responsiveness, characterized as high on-treatment platelet reactivity (HPR), has been shown to be correlated with adverse cardiovascular events after acute coronary syndrome (ACS) and percutaneous coronary intervention (PCI).1234 Platelet activation and aggregation in response to endothelial injury, such as plaque rupture or stenting, is responsible for intracoronary blood clot formation, leading to ischemic heart disease. Moreover, growing evidence suggests that platelets are also important mediators of inflammation and play a central role in atherogenesis itself.56 Therefore, HPR is not only associated with myocardial infarction (MI) or stent thrombosis, but may also be associated with increased coronary atherosclerotic burden. However, the potential relationship between residual platelet reactivity after clopidogrel treatment and the extent and severity of coronary atherosclerosis has not been widely investigated.
Therefore, we conducted an observational study involving consecutive ACS patients who underwent PCI. The purpose of the present study was to evaluate the correlation between HPR and the extent and severity of coronary atherosclerosis. In addition, we evaluated whether HPR after clopidogrel might account for an unfavorable periprocedural outcome in patients with ACS who underwent PCI.
MATERIALS AND METHODS
1. Study population
We analyzed a single center, consecutive non-ST segment elevation ACS and PCI cohort from December 2012 to August 2014. During the study period, 600 consecutive patients were recruited and followed-up during their clinical course to document patient characteristics, acute therapy, PCI data, and hospital outcomes. Exclusion criteria were patients with ST segment elevation MI, the use of other P2Y12 inhibitors instead of clopidogrel, chronic clopidogrel therapy, use of glycoprotein IIb/IIIa inhibitors, previous coronary artery bypass surgery, concomitant proton pump inhibitor use, or lack of laboratory data including platelet reactivity unit (PRU). As a result, 485 patients were analyzed. All patients provided informed consent for the processing of their anonymous data, according to a protocol approved by the Institutional Review Boards of Wonkwang University Hospital.
2. Percutaneous coronary intervention
In all patients, aspirin (300 mg/day) and clopidogrel (300 mg/day) were loaded before the procedure. An intravenous bolus of 5,000 U of unfractionated heparin was given, and then additional heparin boluses were given to maintain activated clotting time >300 s during the procedure. Coronary angiography and stent implantation were performed using standard interventional techniques. Aspirin (100 mg/day), clopidogrel (75 mg/day) and statins were prescribed to all patients after the procedure.
The occurrence of angiographic complications during PCI, including side branch occlusion, slow or no reflow, major dissection, and distal embolization were recorded. Creatine kinase-myocardial band isoenzyme (CK-MB) and troponin T were measured before, at 6 hours, 24 hours and 48 hours after PCI. Additional samples were obtained if the patients showed signs or symptoms of myocardial ischemia.
3. Assessment of platelet reactivity
Platelet reactivity after successful PCI was assessed by VerifyNow P2Y12 assays (Accumetrics, San Diego, CA, USA). Blood samples were taken to measure platelet reactivity at 48 h after 300 mg clopidogrel loading. A washout period was required if platelet glycoprotein IIb/IIIa inhibitors were used, and thus no patients receiving glycoprotein IIb/IIIa inhibitor were enrolled. VerifyNow P2Y12 baseline reactivity, PRU, and P2Y12 percent inhibition were measured to assess platelet function. In this study, platelet reactivity ≥230 PRU was defined as HPR.7
4. End points
The primary end point of the study was the correlation between the extent of atherosclerotic coronary artery disease (defined as coronary artery stenosis >50% in major epicardial vessel and branch) and HPR.
The secondary end point was the occurrence of periprocedural myonecrosis, defined as any increase of cardiac biomarkers above the upper limit of normal or ≥20% increase of elevated baseline value.8 Other secondary end points included periprocedural MI, defined as a postprocedural increase of CK-MB over 3 times higher the normal upper limit in patients with normal baseline enzyme levels. In patients with elevated baseline levels of CK-MB, MI was defined as a subsequent increase that was more than 3 times greater than the baseline CK-MB value and an additional increase in a second sample.
5. Statistical analysis
All measurements were represented as mean±standard deviation or absolute number (percentage). Inter-group analysis was performed using independent t-test and χ2 test, which were conducted using SPSS 19.0 for Window (SPSS Inc., Chicago, IL). The hypothesis of the study was that patients with multi-vessel disease (MVD) would present a 15% greater incidence in the HPR group as compared with patients with single-vessel disease (SVD) after clopidogrel loading. Assuming a 50% incidence of MVD, we calculated that at least 153 patients should be included in each group to provide 80% power to detect between group differences, with a two-sided alpha of 0.05.9 All clinical and procedural variables that showed a significant univariate association with MVD and periprocedural myonecrosis (p<0.1) were entered in a multivariable logistic regression model. For continuous variables, the first or third tertile was used as the cut-off point in logistic regression analysis. Statistical significance was set at p<0.05.
RESULTS
1. Baseline characteristics
The mean PRU value in the overall population was 232.1±87.1, and 260 patients (53.6%) showed HPR (PRU≥230). About 25% of patients presented as MI (non-ST segment elevation MI). Patient characteristics, according to HPR, are shown in Table 1. HPR was observed more commonly in elderly patients, female patients, current smokers, and in patients with previous ischemic stroke. HPR was associated with low hemoglobin and high brain natriuretic peptide levels.
2. HPR and extent of coronary artery disease
The incidence of MVD was higher in patients with HPR than those with no HPR (56.2% vs 45.8%, p=0.023) (Table 2). Patients with MVD showed significantly higher PRU values compared with those with SVD (241.9±86.6 vs. 221.8±86.7, p=0.011; Fig. 1). The PRU values progressively increased with number of diseased coronary arteries (1-vessel disease 221.8±86.7; 2-vessel disease 239.3±90.1; 3-vessel disease 243.4±84.5; p=0.038 by ANOVA). Multivariate analysis revealed that HPR was independently associated with MVD (Odds ratio 1.50, 95% confidence interval 1.01-2.24, p=0.047; Table 3).
3. HPR and periprocedural myonecrosis
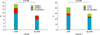
Periprocedural myonecrosis occurred in 58 patients (12.0%) based on any CK-MB elevation and in 172 patients (35.5%) based on any troponin T elevation. Patients with periprocedural myonecrosis showed significantly higher PRU values compared with those without myonecrosis (258.6±94.5 vs. 228.5±85.6, p=0.013). Regarding CK-MB elevation, the incidences of any CKBM elevation (15.0% vs. 8.4%, p=0.026), 2 times the elevation of CK-MB (5.4% vs. 2.2%, p=0.073), and 3 times the elevation of CK-MB (2.3% vs. 0.4%, p=0.129) were higher in patients with HPR compared with those with no HPR (Fig. 2). Regarding troponin T elevation, incidences of any troponin T elevation (40.8% vs. 29.3%, p=0.009), 3 times the elevation of troponin T (14.2% vs. 7.1%, p=0.012), and 5 times the elevation of troponin T (10.8% vs. 5.3%, p=0.030) were significantly higher in patients with HPR compared with those with no HPR. Multivariate analysis revealed that HPR was an independent predictor for periprocedural myonecrosis as defined as any CK-MB elevation or troponin T elevation (Table 4).
DISCUSSION
This study demonstrated that HPR was associated with MVD and periprocedural myonecrosis in patients with ACS and PCI. Thus, platelet reactivity after clopidogrel treatment was associated not only with blood clot formation but also with increased coronary atherosclerotic burden.
Blood platelets actively participate in vascular atherosclerosis. In vitro studies demonstrated that interactions between activated platelets, leukocytes and endothelial cells triggered autocrine and paracrine signals. As a resul, leukocyte recruitment occurred at and into the vascular wall.1011 Moreover, with chemical signaling, direct physical interaction may also support to atherosclerosis, through platelet adhesion molecules and platelet granule release.12 These processes may contribute to foam cell formation and accelerated atherogenesis. Afek et al. reported that antiplatelet therapy could decrease plaque size and improved plaque stability in animal models of accelerated atherogenesis.6 Therefore, increased platelet reactivity may potentiate arterial thrombosis, inflammation, and atherosclerotic progression.
HPR has been defined as a high level of platelet reactivity that is measured during steady state platelet inhibition after receiving a loading dose of an antiplatelet agent.13 Several studies have reported associations between HPR and increased atherosclerotic burden. Keating et al.14 demonstrated that platelet reactivity progressively increases with the number of vascular beds affected by atherosclerosis (cerebral, cardiac, peripheral). Mangiacapra et al.9 reported that MVD was associated with an increased rate of HPR in patients with stable angina. Yun et al. demonstrated that HPR was associated with high plaque burdens and high incidences of fibroatheroma in virtual-histology intravascular study.16 Our findings confirmed these observations and extended them to ACS patients.
Several mechanisms have been described for the suboptimal response to clopidogrel, including genetic, cellular, and clinical factors.17 Increased platelet reactivity was commonly observed in specific clinical scenarios such as ACS, increased body mass index, heart failure, chronic kidney disease and diabetes.1315 In our study conducted in ACS patients, patients with HPR had a higher incidence of hypertension, smoking, previous ischemic stroke, and anemia compared to that in patients without HPR. These results may be caused by different patients' populations, and these different incidences of risk factors according to PRU might have contributed to the higher incidence of MVD in the HPR group.
In our study, HPR was significantly associated with periprocedural myonecrosis, even with different degrees of post-procedural cardiac biomarker elevations. Patti et al.18 reported that HPR (PRU≥240) was associated with a higher incidence of 30-day major adverse cardiac events after PCI; this outcome was mainly driven by an increased risk of periprocedural MI. In view of the more extensive and complex coronary manipulation, patients with MVD might be expected to have a higher risk of periprocedural myonecrosis. Additionally, higher PRU values were observed in MVD patients, and it suggests that suboptimal platelet response to clopidogrel in this clinical setting might be responsible for the higher risk of periprocedural MI. In fact, our study confirmed the results of previous studies which demonstrated that HPR was a strong predictor of periprocedural myonecrosis.91920
Our study has several limitations. This was single center, retrospective study. Clinical follow-ups of the patients were not performed, and the long-term clinical significance of HPR was not evaluated. However, the relation between platelet reactivity and the occurrence of major adverse cardiac events was already reported, regardless of a specific PRU cut-off.72122 Moreover, periprocedural myocardial injury also has been reported as risk factor of major adverse events.23 Our study suggested only correlative associations; the cause-and-effect relationship between platelet reactivity and coronary artery disease burden remains theoretical.
In conclusion, HPR was shown to be associated with MVD and periprocedural myonecrosis in patients with ACS and PCI. It demonstrated the need for more potent antiplatelet strategies in this clinical setting. Further studies are required to define the causal mechanisms between platelet reactivity and the development and progression of atherosclerosis.





 XML Download
XML Download