

 PDF
PDF ePub
ePub Citation
Citation Print
Print


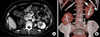
A 71-year-old woman was admitted complaining of left flank pain, and presented with oliguria and hypotension. Pyuria and severe sepsis led to the diagnosis of acute pyelonephritis. An abdominal computed tomography intravenous pyelogram revealed normal-sized kidneys, however, the differentiation between cortex and medulla was poorly determined. The left kidney showed an amorphic, low attenuation lesion that was consistent with acute pyelonephritis (Fig. 1A). Both kidneys were incompletely malrotated and anteriorly facing hila were observed. The renal vessels and ureter were located laterally. The right kidney was 5 cm lower than the left kidney, indicating renal ectopia. Mild dilation was found at the proximal ureter of the left kidney. Additionally, a three-dimensional computed tomography reconstruction image showed anteriorly rotated kidneys (Fig. 1B). The patient initially received piperacillin-tazobactam empirically, then switched to cefotaxime after detecting an E. coli infection in the bloodstream. Three days later, her hemodynamic state had improved, and she was released from the intensive care unit.
Malrotation of the kidney may cause partial obstruction of the ureteropyelic junction, which can cause increased incidences of urolithiasis and infection.1 In our case, the patient had a dilated left ureter (not shown) associated with mild obstruction due to a ureteral deformation and renal malrotation. We assumed that these abnormalities were responsible for her recurrent urinary tract infections as well as the acute pyelonephritis with septic shock. To our knowledge, this is the first case report of a patient diagnosed with septic shock due to acute pyelonephritis associated with renal malrotation. Furthermore, in patients with recurrent urinary tract infections, thorough image evaluation and assessment of risk factors is important. The abdominal computed tomography intravenous pyelogram is a demonstrably useful diagnostic evaluation tool in patients with renal anomalies.
 XML Download
XML Download