

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Metabolic alkalosis (MA) is common acid-base disturbance encountered in hospitals, and is present in 51% of patients with an abnormal acid-base status.1 Severe MA, indicated by a pH value greater than 7.55, is a serious, emergent condition and rapid correction is mandatory. We report here a case of extreme MA associated with gastrostomy and complicated by seizure and stupor. Although the patient was hydrated adequately using a normal saline solution, the MA persisted. Using hemodialysis (HD) therapy with a simple formula of conventional dialysate bicarbonate (30 mmoL/L), we successfully treated the extreme MA associated with gastrostomy.
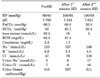
A 30-year-old man presented to the emergency room with seizure and altered mental status. He had a preexisting gastrostomy tube because of advanced gastric cancer and carcinomatous peritonitis. Brain computed tomography (CT) excluded cerebral bleeding and ischemia, but an abdominal CT showed dislodgement of the gastrostomy tube tip on the gastric fundus. Laboratory tests showed an elevated serum pH of 7.709, partial pressure of arterial carbon dioxide (PaCO2) of 66.5 mmHg, partial pressure of arterial oxygen (PaO2) of 55.5 mmHg, bicarbonate (HCO3−) of 82 mmoL/L, and base excess (BE) of 62.2 mmoL/L (Table 1). In addition, potassium, sodium, and chloride levels were low whereas blood urea nitrogen, creatinine, and magnesium levels were high. Hemoglobin was 10.5 g/dL and hematocrit was 31.5%, while urine sodium was 8 mmoL/L and urine osmolality was 410 mOsmol/kg. With this evidence, we diagnosed severe hypochloremic MA and acute kidney injury associated with the volume depletion caused by the gastrostomy tube malposition. Intravenous application of sodium chloride 0.9% (6 L) and potassium did not improve the acid-base state, electrolyte homeostasis, or kidney function. Emergent HD with a dialysate bicarbonate concentration of 30 mmoL/L was performed for 4 hours using a Gambro Phoenix dialysis machine (Gambro AB, Stockholm, Sweden), which could only make variant bicarbonate concentrations of 30 to 40 mmoL/L. The post-HD arterial blood gas analysis showed a pH of 7.424, PaCO2 of 68.0 mmHg, HCO3− of 43.7 mmoL/L, and BE of 18.0 mmoL/L. The patient also showed improved mental status and an improved laboratory test profile (pH=7.621, PaCO2=26.0 mmHg, PaO2=170.4 mmHg, HCO3−=26.2 mmoL/L, BE=5 mmoL/L) after the second HD session.
Successful treatment for MA depends on prompt recognition of the underlying disorder and rapid correction. Wilson et al. reported that a pH value of 7.54 to 7.56 resulted in a mortality rate of 45%, while a pH value of 7.65 to 7.70 was associated with a mortality rate of 80%.2 Precipitating factors such as nasogastric suction, vomiting, and alkali ingestion or infusion are usually present in the most severe cases,3 and gastric alkalosis, caused by profound vomiting or continuous gastric suction, accounts for the most severe form of MA. However, a serum bicarbonate concentration greater than 55 mmoL/L has rarely been observed.4 Furthermore, in patients with severe MA, which usually presents with tetany, seizure, delirium, or stupor, an emergent correction is mandatory.56 However, in patients with renal failure, a high serum bicarbonate concentration can be treated through titration with hydrochloric acid or renal replacement therapy.5 While the titration method is limited because it is toxic, time-consuming, and not commercially available, renal replacement therapy using hemodialysis (HD) with a specially formulated low-bicarbonate, low-acetate, or acid dialysate solution has been shown to be successful.47 However, few studies have examined the role of normal bicarbonate dialysate in ameliorating severe MA.8 Our successful experience shows that conventional HD with conventional bicarbonate dialysate (30mmoL/L) is a convenient and effective modality in a severe MA case.
In conclusion, gastrostomy tube malposition may induce extreme MA, and a conventional HD with even a higher bicarbonate concentration (30mmoL/L) than normal is a safe and effective intervention in such cases.
 XML Download
XML Download