

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Statin therapy is a key treatment for patients with coronary heart disease (CHD). Multiple randomized trials have shown beneficial effects of statin therapy for reducing the rate of recurrent myocardial infarction (MI), coronary disease mortality, the need for revascularization, and stroke.12
Inhibitors of the renin-angiotensin system (RAS) such as angiotensin converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARB) are important drugs for patients with any potential causes of systolic heart failure (HF). RAS blockers improve morbidity and mortality in these patients and also has been recommended for MI patients with HF or left ventricular ejection fraction (LVEF) less than 40%.345
The post-hoc analysis of a GREACE (Greek Atorvastatin and Coronary Heart Disease Evaluation) study showed the 'synergic effect' of statins and ACE inhibitors in reducing vascular events in patients with CHD. Aggressive statin use in the absence of an ACE inhibitor also substantially reduced cardiovascular events. Treatment with an ACE inhibitor without statins use did not significantly reduce clinical events in comparison to patients not treated with an ACE inhibitor.6
The aim of the present study is to compare these two drugs, statins and RAS blockers, and to assess which drugs would be more effective for the reduction of major adverse cardiac and cerebrovascular events (MACCEs) in IHF patients who underwent percutaneous coronary intervention (PCI) for acute myocardial infarction (AMI).
MATERIALS AND METHODS
1. Patient population
The study population was selected from the Korea Acute Myocardial Infarction Registry (KAMIR). This is a Korean prospective multicenter data collection registry reflecting real-world treatment practices and outcomes in Asian patients diagnosed with AMI.7 The registry includes 53 communities and teaching hospitals with facilities for primary PCI and on-site cardiac surgery. The KAMIR was supported by a research grant from the Korean Circulation Society in commemoration of its 50th anniversary. Data was collected by a trained study coordinator using a standardized case report form and protocol. The study protocol was approved by the ethics committee at each participating institution.
Between November 2011 and July 2014, 9,369 AMI patients were enrolled. Inclusion criteria for the present analysis were patients aged over 18, diagnosed as AMI with a LVEF <40%, and who underwent PCI. The exclusion criteria for the study were patients who had died during hospitalization druing the index procedure; were lost to follow-up; and lacked information for the LVEF.
From the registered patients, a total of 804 patients were included in this analysis (Fig. 1). Patients were divided into four groups according to the documentation of drugs prescribed at discharge [Group I, combination of statins and RAS blockers (n=611), Group II, statins alone (n=112), Group III, RAS blockers alone (n=53), and Group IV, neither treatment (n=28)].
2. PCI procedure
PCI was performed using a standard technique. All patients received a 300 mg loading dose of aspirin and a 300 to 600 mg loading dose of clopidogrel before PCI unless they had previously received these antiplatelet drugs. Anticoagulation during PCI was performed according to current practice guidelines established by the Korean Society of Interventional Cardiology. The decision for thrombus aspiration, pre-dilatation, direct stenting, and post-adjunctive balloon inflation, and the administration of glycoprotein IIb/IIIa inhibitors were left to the discretion of individual operators. Drug eluting stents were used without restrictions. The duration of the dual antiplatelet therapy was determined by the operators.
3. Definitions and outcomes
MI was diagnosed by the presence of a characteristic clinical presentation, serial changes on electrocardiogram suggesting infarction, and increased cardiac enzymes. ST-segment elevation myocardial infarction (STEMI) was diagnosed as a suggestive symptom with a ST-segment elevation >2 mm in ≥2 precordial leads, ST-segment elevation >1 mm in ≥2 limb leads, or a new left bundle branch block on the 12-lead electrocardiogram with a concomitant increase of at least one cardiac enzyme. Heart failure is defined as decreased ventricular function and ischemic haert failure is described as heart failure with any ischemic cause such as coronary artery disease. A left ventricular ejection fraction of <40% by echocardiogram is diagnosed as heart failure. The study end point was the time beginning with the first MACCEs lasting for 2 years. MACCE included death of cardiac origins, non-fatal MI, repeated PCI, the need for a coronary artery bypass graft, and a cerebrovascular accident.
4. Statistical analysis
Baseline characteristics and angiographic characteristics were summarized with the use of descriptive statistics, between-group differences were assessed by means of the Kruskal-Wallis test. All other data, which were non-parametrically distributed and are expressed as median values with inter-quartile ranges, were analyzed with the use of the Kruskal-Wallis test for between-group comparisons. Survival curves were constructed with Kaplan-Meier estimates and compared with the log rank test; data was censored at the time of the last visit.
The Cox proportional-hazards model was used to identify factors associated with an increased risk of MACCEs. Factors associated with MACCEs with a p value of less than 0.20 in the univariate analysis were entered in the multi-variate model, and non-significant factors were removed by means of a backward-selection procedure. All statistical analyses were done with SPSS 18.0 (Statistical Package for the Social Sciences, SPSS-PC Inc, Chicago, IL, U.S.A.). A p value<0.05 was considered statistically significant.
RESULTS
1. Baseline clinical characteristics
Baseline clinical characteristics are shown in Table 1. There were no significant differences among the treatment groups except for those with a history of diabetes mellitus, Killip class ≥III on admission, an estimated glomerular filtration rate (eGFR), total cholesterol and low density lipoprotein (LDL) cholesterol levels, and the proportion receiving β blockers with respect to the overall demographic characteristics. Group IV had a highest prevalence of diabetes mellitus and the lowest eGFR. Group III and IV had higher rates of Killip class ≥III on admission.
2. Procedural characteristics
The coronary angiographic and procedural characteristics are shown in Table 2. The prevalence of left anterior descending artery or multi-vessel involvement did not differ, and the rate of severe lesion and pre-PCI Thrombolysis in Myocardial Infarction (TIMI) flow were also similar and there were no significant differences in stent diameter or length among the four groups. However, Group IV had the lowest proportion of stent use and the lowest rate of post-procedural TIMI flow with a grade of 3.
3. Clinical outcomes
The median duration of follow-up was 362 days (interquartile range 186-686). Table 3 shows the cumulative clinical outcomes of the study groups. MACCEs occurred in 48 patients (7.9%) in Group I, in 16 patients (14.3%) in Group II, in 3 patients (5.7%) in Group III, and in 7 patients (21.4%) in Group IV (p=0.013).
Fig. 2 shows a Kaplan-Meier curve for MACCE-free survival. The four groups did not show the same survival curves (p=0.005). In post-hoc analysis, Group I showed a better outcome compared with Group II (p=0.047) or Group IV (p=0.011), but did not show a difference compared with Group III (p=0.634). Group III also showed better outcome compared with Group IV (p=0.011). All other inter-group analysis showed no significant difference between Group II and III (p=0.130), and between Group II and IV (p=0.183).
4. Independent predictors of MACCE
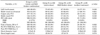
Table 4 shows the univariate analysis of the independent predictors for the development of a MACCE. Age, previous history of hypertension, eGFR, body-mass index, multi-vessel involvement, STEMI, and use of RAS blockers were also associated. Table 5 shows the multivariate analysis of the independent predictors for development of MACCE. The use of RAS blockers [Odds ratio (OR) 0.469, 95% confidence interval (CI) 0.285-0.772, p=0.003], eGFR (OR 0.989, 95% CI 0.981-0.997, p=0.005), multi-vessel involvement (OR 1.810, 95% CI 1.049-3.125, p=0.033), and a previous history of hypertension (OR 1.691, 95% CI 1.015-2.817, p=0.044) were the independent predictors of MACCEs in patients with IHF who underwent PCI for AMI.
DISCUSSION
This study was analyzed retrospectively using the KAMIR data. This gives a comprehensive view of the contemporary treatments and outcomes of patients with AMI in Korea. The present study found that in patients with AMI with reduced left ventricular systolic function who underwent PCI, the use of RAS blockers was associated with a 53% reduction in the risk of cardiac death, MI, revascularization, or a cerebrovascular accident. However. statin use did not show a reduction of the incidence of MACCEs.
To analyze the results regarding the MACCE-free survival curve, the ratio of the patients who suffered a MACCE in Group IV was much higher than that in other groups. As mentioned above, Group IV had a higher prevalence of diabetes mellitus, higher rates of Killip class ≥III, lower eGFR, lower LDL cholesterol level, lower rates of stent use, and lower rates of post-PCI TIMI flow III. Although there was no statistical difference among the 4 groups, Group IV had a higher prevalence of hypertension and heart failure, as well as a higher rate of female patients than Group I or II. These differences of the baseline characteristics might make have led to a poorer prognosis in Group IV. The highest number of non-cardiac death and the lowest frequency of prescribed β blockers in Group IV indicated that Group IV patients had poor general health conditions such as low blood pressure or slow heart rate. The small number of patients in Group IV, only 28 persons, prevents the results from this study to be widely generalized. After excluding Group IV, comparing Group I with Group II and Group I with Group III. RAS blockers showed a statistically significant beneficial effect (p=0.047) but the statin dose did not (p=0.638).
ACE inhibitors can reduce morbidity and mortality due to major cardiovascular events in patients with left ventricular systolic dysfunction after AMI.8910 The effectiveness of ARB showed weaker results than that of ACE inhibitors. However, in the Valsartan in Acute Myocardial Infarction (VALIANT) trial, valsartan was superior to captopril in patients with left ventricular systolic dysfunction after AMI.11 Therefore, the guidelines recommend that ACE inhibitors should be started and continued in all patents with a LVEF less than 0.40 after AMI and ARBs should be considered as an alternative in patients who are intolerant to ACE inhibitors.45 Recent studies show that ARB is better than ACE inhibitors in some specific subgroups such as patients with STEMI with preserved left ventricular systolic function.12 In the present study, RAS blockers reduced MACCEs effectively compared to statin use alone or neither using RAS blockers nor statins. As RAS blockers have similar mechanisms, we congregate ACE inhibitors and ARB into one group. All ARBs look the same and show a class effect, but ARBs can be classified as insurmountable or surmountable. Insurmountable ARBs were more effective on long-term clinical outcomes than surmountable ARBs in patients with AMI, those with a LVEF greater than 40% with a low Killip class, or those with normal renal function.13 Further studies are needed to evaluate the effectiveness of rhw subclasses of ARBs.
Statins also lower the risk of coronary heart disease death, recurrent MI, stroke, and the need for coronary revascularization in patients stabilized after an acute coronary syndrome.1415 All patients with coronary heart disease should receive long-term intensive lipid lowering therapy with a statins.45 When it comes to patients with HF, however, the efficacy and safety of statin therapy is still controversial. Large observational and post hoc analyses from large clinical trials have suggested that statins could provide clinical benefits to patients with HF.161718 However, two recent, large, randomized controlled trials have demonstrated that rosuvastatin does not affect clinical outcomes in patients with chronic HF, even in ischemic cases.1920 So the current guidelines do not recommend statins solely for HF in the absence of other indications for their use.3 Some concerns have been raised that the results cannot be generalized to all patients with HF because the enrolled patients had moderate to severe disease and were older, only low to moderate doses of rosuvastatin were tested, and ischemic events occur less frequently in patients with HF compared with the broad population of patients with established cardiovascular disease.21 More recently, in a large scale prospective propensity score matched cohort study, statins were associated with improved outcomes, specifically in the presence of ischemic heart disease.22 A meta-analysis also found that statin therapy significantly decreases the rate of hospitalization for worsening HF and increased left ventricular ejection fraction, though it does not decrease all-cause or cardiovascular mortality compared with placebo.23 Statin therapies for hypercholesterolemia and primary and secondary prevention of CAD has been established, however, their effects on patients with HF have remained unclear. In the present study, statins did not show any beneficial effects in the prevention of the occurrence of future events. However, there was a small number of patients who did not use statins (81 patients, 10% of total patients). Therefore, a large, prospective, randomized trial is needed to determine the effectiveness of statin therapy for ischemic heart failure.
There were several limitations to this study. First, this was a non-randomized study based on a prospective, observational registry. Therefore, a selection bias was largely unavoidable. The baseline demography showed the differences in the 4 groups. RAS blocker users more frequently prescribed β blockers as well. In this study β blockers were not shown to be statistically effective (OR 0.843, 95% CI 0.488-1.456, p=0.547), but β blockers are also a key drug in patients with HF and proven to reduce mortality. β blockers may induce some or all of the positive effects of RAS blockers, especially the prevention of MACCEs. Although most confounders were included in the multivariate analysis, it is possible that some potential bias was included. Second, the types and doses of the prescribed statins were variable. There were four different types of statins and each had three or four variation of dosage. Third, KAMIR data does not have information on why physicians did not prescribe a RAS blocker or statin, because of the limitations of our database. Finally, a median follow-up of 12-months might be too short to conclusively determine the long term efficacy of treatment. These findings support the need for prospective, randomized, blinded, placebo-controlled trials to determine the effectiveness of statin therapy for IHF.
RAS blockers showed beneficial effects in patients with IHF who underwent PCI for AMI. But statins were not associated with better clinical outcomes compared with RAS blockers or neither treatment.






 XML Download
XML Download