

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Staphylococcus aureus bacteremia is potentially fatal. It is rare complication of in vitro fertilization and embryo transfer (IVF-ET). This is the first reported case of successful term delivery following S. aureus bacteremia with vertebral osteomyelitis after IVF-ET.
CASE REPORT
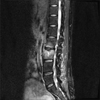
A 30-year-old, 16-week primipara woman visited an obstetric department with complaints of pain in the bilateral pelvis and lower back over the past 3 weeks. She had a history of ultrasound-guided transvaginal oocyte retrieval (TVOR) for IVF 14 weeks earlier; 3 days after the TVOR, embryo transfer was performed. After this, she used vaginal progesterone suppositories (200 mg twice a day) for 6 weeks prior to hospitalization. Upon admission, her vital signs were as follows: blood pressure, 113/76 mm Hg; heart rate, 95 beats/min; respiration, 20 breaths/min; and temperature, 37.6℃. A complete blood cell count, routine chemistry, urinalysis, urine culture, and blood culture were ordered on admission. Of these results, abnormal values were reported for the white blood cell count (10.33×103/mL), hemoglobin (10.6 g/dL), C-reactive protein (6.43 mg/dL), and erythrocyte sedimentation rate (90 mm/h). Lumbar spine X-rays showed nonspecific findings. Lumbar spine magnetic resonance imaging showed high-intensity-signal changes of the second and third lumbar vertebrae (Fig. 1), suggesting infectious spondylitis. Thus, a spinal biopsy was performed, and cefazolin was initiated at 2 g every 8 h.
The results of the blood and spinal biopsy cultures and antibiogram showed S. aureus that was sensitive to penicillin, methicillin, clindamycin, ciprofloxacin, and vancomycin. Intravenous cefazolin (6.0 g/day) was continued. Amniotic fluid cultures did not show any bacteria. The infant was appropriate in size for her gestational age and had no deficits.
On day 7, a transthoracic echocardiogram showed a normal resting echocardiogram and no vegetations on the mitral or aortic valves. On day 9, blood cultures were repeated, and no S. aureus growth was observed. On day 12, her pelvic and lower back pain had improved.
Cefazolin was continued for 6 weeks. The patient recovered completely and was discharged on the 44th hospital day. Four months later, she delivered a healthy girl by normal delivery at 38 weeks and 4 days. She experienced no sequelae or recurrence of the infection.
DISCUSSION
The rates of infectious complications in IVF are low at <1%. Some reports have presented ovarian abscesses or pelvic abscesses complicating IVF.1 However, there is only one report of vertebral osteomyelitis as a complication of IVF.2 In that case, a woman developed vertebral osteomyelitis after ultrasound-guided TVOR.2 This case assumed that the route of infection was direct inoculation of vaginal organisms carried to the fifth lumbar vertebra by the needle, and the vertebral osteomyelitis pathogen in this case was Escherichia coli.2
In most instances, vertebral osteomyelitis results from direct inoculation, contiguous spread from an infection in a nearby organ, or hematogenous seeding.3 S. aureus is the most common pathogen in bacterial vertebral osteomyelitis, followed by E. coli.3
In our patient, the pathogen was methicillin-susceptible S. aureus, which grew in both the blood and spinal biopsy cultures. We presumed two mechanisms of the vertebral osteomyelitis in our case: direct inoculation during TVOR, as in the previous case of Almog et al.,2 and hematogenous seeding.
S. aureus is one of the most common pathogens of both community- and health care-associated infections, which result in considerable morbidity and mortality.4 S. aureus bacteremia may lead to various local complications or distant metastatic infections.5 Frequent sites of distant metastatic infections include the joints, bones, epidural space, intervertebral discs, and cardiac valves.5 The anterior nares and skin are the major reservoirs of S. aureus in humans.4,5 In patients with S. aureus bacteremia, there is a strong correlation among strains colonizing the anterior nares, strains isolated from foci of infection, and strains isolated from blood, which suggests that S. aureus bacteremia may have an endogenous origin.4 Other investigators studied the prevalence of S. aureus colonization in pregnancy at various anatomic sites and showed by use of recto-vaginal cultures that 17% of women (507/2,963) were positive overall for S. aureus colonization.6,7 Our patient underwent TVOR, injection of various drugs, and daily insertion of vaginal progesterone suppositories. We presume that during this process, S. aureus colonized in the vagina or on the skin could have invaded the bloodstream and resulted in S. aureus bacteremia. Unfortunately, we did not identify S. aureus colonization in her vagina or on her skin or anterior nares.
This is the first reported case of S. aureus bacteremia with vertebral osteomyelitis after IVF. Our case is even more significant because of its occurrence during pregnancy after IVF.
There have been some reports of S. aureus infection in pregnant women who did not undergo IVF.8,9,10 One previous study reported a primary psoas muscle abscess caused by methicillin-susceptible S. aureus in a pregnant woman. In that case, the patient was treated with cefazolin injection (6 g/day) for 6 weeks. Another case reported nosocomial methicillin-resistant S. aureus endocarditis with a splenic abscess in a pregnant woman, and intravenous teicoplanin was continued for 6 weeks after surgery. In another case, nafcillin, vancomycin, and daptomycin were used to treat methicillin-susceptible S. aureus endocarditis in a pregnant woman. In our patient, intravenous cefazolin was continued for 6 weeks without surgery during her pregnancy, and she fully recovered and delivered a healthy girl.
In conclusion, this is the first reported case of S. aureus bacteremia with vertebral osteomyelitis in a pregnant woman after IVF. Because infertility treatments are increasing, the number of infectious complications of IVF will likely increase. S. aureus bacteremia can be a serious complication of IVF. If patients who have undergone IVF complain of back pain, vertebral osteomyelitis should be considered.
 XML Download
XML Download