

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Immunoglobulin G4-related disease (IgG4-RD) is a fibro-inflammatory systemic disease characterized by elevation of serum IgG4, dense fibrotic infiltration of IgG4-positive plasma cells, and obliterative phlebitis.1 Because IgG4-RD affects almost all organ systems, the disease may be of interest not only to internists but also to other physicians.2 Almost all IgG4-related kidney disease (IgG4-RKD) is combined with tubulointerstitial nephritis (TIN) and renal dysfunction due to hydronephrosis and obstructive nephropathy.3 Here, we describe a case of IgG4-RD involving the kidneys, bladder, and ureter as well as the thyroid, submandibular, and lacrimal glands without TIN, hydronephrosis, or renal dysfunction.
CASE REPORT
A 64-year-old female was referred to Gachon University Gil Medical Center for further evaluation of incidentally detected bilateral renal masses. She had a history of a partial thyroidectomy due to a thyroid mass, which was diagnosed as benign, and she was taking levothyroxine. A physical examination showed symmetrically swollen lacrimal and submandibular glands but no abnormal tenderness. Quite well-demarcated, nodular, and movable swollen eyes were noted, but no visual field defects or limitations in ocular movement were detected. Palpable, nodular, and movable submandibular gland masses without tenderness were also present.
Her laboratory data showed a white blood cell count of 7.24×103/mm3, a hemoglobin level of 12.0 g/dL, a platelet count of 349×103/mm3, a serum blood urea nitrogen level of 17.0 mg/dL, a creatinine level of 0.7 mg/dL, an erythrocyte sedimentation rate of 39 mm/h, and a high-sensitivity C-reactive protein level of 0.05 mg/dL. A white blood cell count of 11 to 20 and a red blood cell count of 3 to 5 were shown in her urinalysis, but the results of a urine gram stain were negative.
Her serum IgG level was increased to 2,052 mg/dL, and the serum IgG4 level was 1,281 mg/dL (Fig. 1). In addition, her serum total IgE level was also increased to 1,050 U/mL. Other serum Ig levels were normal, including those of IgA and IgM. Serum C3 (78 mg/dL) and C4 (25 mg/dL) levels were within the normal range.
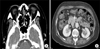
A computed tomography (CT) scan of the orbit and chest demonstrated enlarged bilateral lacrimal glands with enhancement (Fig. 2A), a low-density nodule in the left lobe of the thyroid gland and right lobectomy status (Fig. 2B), but no evidence of a mass lesion in either submandibular gland. We consulted ophthalmology and otolaryngology because of concern over a neoplasm. Lacrimal and submandibular gland biopsies were recommended but the patient refused owing to the low overall estimated risk of malignancy. An abdominal CT scan showed renal pelvic, calyx, and left pelvic masses extending into the upper ureter, suggesting urothelial cell carcinoma (Fig. 2C). The results of urine cytology were negative for malignancy. A bladder mass was detected on cystoscopy at the trigone, suggesting a bladder tumor. No filling defect was found on ureteroscopy. Because a malignancy could not be ruled out, an ultrasonogram-guided biopsy was performed on the pelvocalyceal masses. A histopathological examination was negative for malignancy (Fig. 3A) but showed dense lymphoplasmacytic infiltration with an increased number of IgG4-positive plasma cells. IgG4 immunostaining revealed >25 IgG4-positive cells per high-power field (HPF) (Fig. 3B). However, kidney biopsy showed relatively well-preserved glomeruli and tubulointerstitium (Fig. 3C).
We initially prescribed 30 mg oral prednisolone daily for 4 weeks with a subsequent decrease in dosage by 10 mg every 4 weeks. The patient was maintained on low-dose steroid therapy with serum IgG4 level monitoring. A follow-up CT scan and IgG4 level test were performed at the appropriate time. The sizes of the lacrimal gland, the submandibular gland (Fig. 4A), and the parapelvic masses in both kidneys slowly diminished (Fig. 4B). The IgG4 level also decreased with systemic steroid treatment, which has been maintained with no recurrence.
DISCUSSION
IgG4-RD is recognized as a fibro-inflammatory systemic disease with the following features: extensive IgG4-positive plasma cell infiltration in various organs, tumefactive lesions, and an elevated serum IgG4 concentration.1 IgG4-RD was first described in a pancreatic lesion and was thus called autoimmune pancreatitis (AIP), but is now considered to include inflammatory lesions in almost every organ.2 The clinical manifestations of IgG4-RD are diverse, including AIP, sclerosing cholangitis, sialadenitis, cholecystitis, retroperitoneal fibrosis, TIN, interstitial pneumonia, prostatitis, inflammatory pseudotumor, and lymphadenopathy.3 The pancreas is recognized as one of the most commonly involved organs, although some IgG4-RD cases without pancreatic involvement have also been reported.1
The dominant feature of IgG4-RKD is TIN characterized by plentiful IgG4-positive plasma cells with storiform fibrosis. However, several glomerular lesions are also concurrent with TIN. Most IgG4-RKD cases have shown prior pancreatic involvement, but isolated IgG4-RKD has also been reported.4 Several radiological findings within the kidneys, including the renal parenchyma and pelvis, have also been used to diagnose IgG4-RKD.5 It is difficult to distinguish a renal or a ureteral malignancy from a nonneoplastic lesion by an imaging study alone, however. Urine cytology is simple and convenient, but is often not the correct tool for diagnosing cancer.6 Therefore, it is important to consider the possibility of diagnosing IgG4-RD by preoperative cytology or ureteroscopic biopsy. Comprehensive diagnostic criteria for IgG4-RKD are proposed in patients with (i) the presence of kidney damage or dysfunction with either elevated serum IgG or IgE or hypocomplementemia; (ii) abnormal radiological findings in the kidneys, such as multiple low-density lesions on enhanced CT, diffuse enlargement of kidneys, a hypertrophied renal pelvis, or a hypovascular solitary renal mass; (iii) elevated serum IgG4 level (>135 mg/dL); (iv) histological renal findings such as dense lymphoplasmacytic infiltration by >10 IgG4+ plasma cells/HPF, >40% IgG4+/IgG+ plasma cells, or characteristic fibrosis with abundant lymphocytes and/or plasma cells; and (v) histological findings in extrarenal organs.2 Our patient had kidney and calyces masses, but no TIN or hydronephrosis, which might be easy to misdiagnose as a malignancy, thus leading to surgery. She had elevated serum IgG4 (1,281 mg/dL), masses in both renal pelvocalyceal systems, and dense lymphoplasmacytic infiltration by >25 IgG4+ plasma cells/HPF. Thus, our patient was compatible with the IgG4-RKD diagnostic criteria even without the common manifestation of TIN, and the disease subsided dramatically after corticosteroid therapy without surgical treatment.
Chronic sclerosing sialadenitis, which was formerly known as Kuttner's tumor, presents with a firm swelling of the salivary gland lasting >3 months.1 Mikulicz's disease is characterized by persistent symmetrical swelling of the orbits, including the lacrimal, parotid, and submandibular glands, and was considered to be a subtype of Sjögren's syndrome for some time but is now regarded as a distinct disease because it features a high serum IgG4 level and a dense lymphoplasmacytic infiltrate rich in IgG4-positive plasma cells with fibrosis in affected glands.2 Our patient was diagnosed with IgG4-RD because of symmetrical swelling of the lacrimal, submandibular, and salivary glands for >3 months and an elevated serum IgG4 level (1,281 mg/dL).2
Thyroid gland involvement is part of the IgG4-RD spectrum. Patients with AIP occasionally manifest accompanying hypothyroidism. In a previous report, 70 cases of Hashimoto's thyroiditis were divided into 19 IgG4-related cases and 51 non-IgG4-related cases.7 Hypothyroidism in patients with AIP may indicate IgG4-related thyroiditis. Hence, physicians may misdiagnose the disease as Hashimoto's thyroiditis because of the overlapping symptoms and laboratory findings. Riedel thyroiditis is also considered a component of the multifocal fibrosclerosis of IgG4-RD. Histopathological features remain the gold standard for diagnosing Riedel and Hashimoto's thyroiditis. Our patient did not undergo a biopsy but she had hypothyroidism and a high IgG4 level, symmetrical submandibular and lacrimal gland enlargement, and a thyroid nodule on neck CT. Moreover, the thyroid nodule also responded to corticosteroid therapy. Therefore, we could assume that the previously removed thyroid nodule of this patient might also have been related to IgG4-RD.
Most IgG4-RD patients respond quite well to corticosteroid therapy. Therefore, steroids should be regarded as first-line therapy, although well-designed controlled trials have not been performed and steroid therapy protocols are inconsistent among countries and institutions.1 Among 19 Japanese patients with IgG4-TIN, 18 (94.7%) patients showed rapid improvement in renal function, radiologic findings, and hypocomplementemia 1 month after initiation of corticosteroid therapy.5 These results suggest that corticosteroid treatment may be insufficient as the first-line therapy and that a large-scale prospective study is necessary to determine more effective treatment strategies in patients with IgG4-RD. In our case, the patient had no signs of renal dysfunction or hydronephrosis. If hydronephrosis and renal dysfunction are present, an indwelling ureteral stent should be considered.
A decrease in the serum IgG4 level and reduced numbers of IgG4-positive plasma and lymphoid cells in involved organs commonly accompany patients who respond well to corticosteroid therapy.8 The serum IgG4 concentration could be utilized as an IgG4-RD biomarker and may also be useful for predicting relapse and evaluating extrapancreatic lesions.9 Even though elevation of IgG4 concentrations were commonly observed after initiation of steroid withdrawal, physicians should promptly consider clinical evidence of other disease if they recognize a significant increment of the serum IgG4 level.10
In summary, we have described a case of IgG4-RD involving multiple organs in which we monitored the serum IgG4 level during diagnosis and treatment. This type of systemic involvement and consecutive monitoring of the serum IgG4 level is the first such case report in Korea. Hence, clinicians should consider the possibility of IgG4-RD in cases of multiple nodular organ involvement, which can be confused with malignancy, to avoid unnecessary surgery.



 XML Download
XML Download