

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Proctitis is an inflammation of the mucosa of the rectum and is most commonly associated with inflammatory bowel diseases (IBDs), including Crohn's disease and ulcerative colitis.1 However, proctitis has other noninfectious causes, such as radiation-associated proctitis, ischemic proctitis, and diversion colitis, and several infectious causes. Frequently reported pathogens of infective proctitis include Neisseria gonorrhoeae, Chlamydia trachomatis, Treponema pallidum, and herpes simplex virus, which involve sexually transmitted diseases (STDs).1 Among these, C. trachomatis is the second most common bacterial pathogen of proctitis followed by N. gonorrhoeae.1 Rectal infection of C. trachomatis primarily occurs in men who have sex with men.2 Because the clinical presentations and endoscopic features of chlamydial proctitis resemble those of IBD, chlamydial proctitis can be misdiagnosed as IBD.34 There have been reported cases of chlamydial proctitis in the United States and Europe that were initially misdiagnosed as IBD. However, only one case of severe chlamydial proctitis has been reported in Korea, which was misdiagnosed as rectal cancer.5 Herein, we report a case of chlamydial proctitis that was initially misdiagnosed as IBD.
CASE REPORT
A 20-year-old man presented with anorectal pain and bloody rectal discharge for 2 months. He had visited a local outpatient clinic and was referred to us for suspected IBD on colonoscopy. He had neither a notable medical nor family history. He had not travelled anywhere recently. He was not taking any medication including antibiotics. He did not complain of other gastrointestinal symptoms, such as diarrhea and vomiting. He did not have systemic symptoms, such as general weakness, fever, or weight loss. He did not have a history of radiation therapy. On physical examination, his abdomen was soft, and there were no palpable lymph nodes in the inguinal area. Neither anal fissures nor hemorrhoids were observed on the rectal examination.
The results of laboratory studies were as follows: white blood cell count, 8,400/mm3; hemoglobin, 14.9 g/dL; platelets, 237,000/mm3; aspartate aminotransferase, 38 IU/L; alanine aminotransferase, 18 IU/L; total bilirubin, 0.8 mg/dL; total protein, 7.3 g/dL; albumin, 4.3 g/dL; blood urea nitrogen, 9.8 mg/dL; creatinine, 0.9 mg/dL; C-reactive protein, <0.01 mg/dL; ESR, 12 mm/hr. VDRL was nonreactive and HIV Ag/Ab were negative. No Shigella or Salmonella was grown from the stool culture and the result of a test for Clostridium difficile toxin was negative.
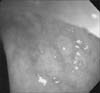
On colonoscopy, hyperemic and granular nodules were observed on the rectal mucosa (Fig. 1A), and a 7-mm whitish polypoid mass was observed in the anal canal, which was histologically confirmed as condylomata acuminata. Histologic findings of the rectal biopsy showed chronic proctitis with lymphoid follicles and lymphocyte aggregations. No granuloma or cryptitis was observed (Fig. 1B, 1C).
Because these findings were not consistent with the typical findings of IBD, we obtained an additional sexual history and found out that he had experience of engaging in homosexual practice. We performed an additional PCR test for C. trachomatis, N. gonorrhoeae, Mycoplasma genitalium, and Ureaplasma urealyticum with a rectal swab and serologic tests for C. trachomatis. The PCR results were positive only for C. trachomatis. In serologic tests, IgM Ab and IgG Ab for C. trachomatis were positive and negative, respectively. Finally, he was diagnosed with chlamydial proctitis. However, molecular typing of the serovars of C. trachomatis was not performed, because testing tools for serovars of C. trachomatis were not available in our center. Also, the patient was not strongly suspicious for lymphogranuloma venereum (LGV) proctitis, because his symptoms and endoscopic findings did not correspond to severe inflammation. He was treated with intramuscular ceftriaxone 250 mg in a single dose and doxycycline 100 mg orally twice daily for 7 days and was discharged without symptoms. In addition, his sexual partners were recommended to visit the hospital. After 2 months, he had no lower abdominal symptoms and his endoscopic findings were improved (Fig. 2).
DISCUSSION
C. trachomatis is a gram-negative bacterium that is one of the most frequently reported bacterial pathogens of STDs. All 15 serovars of C. trachomatis can cause proctitis. Whereas non-LGV proctitis caused by serovars A-K produces mild inflammation confined to the rectal mucosa and causes few or no symptomatic infections, LGV proctitis caused by serovars L1-3 produces more severe inflammation. 4678 Endoscopic findings of chlamydial proctitis reveal a great variety of rectal lesions, from mild erythematous and friable mucosa to deep ulcers or granulomas with mucopurulent exudates.39 These endoscopic features are difficult to differentiate from IBD. In advanced stages of LGV proctitis, transmural inflammation and rectal strictures can develop, further resembling IBD. On histologic study, lymphoplasmacytic infiltrates, cryptitis, crypt abscess, and granuloma are often observed.3 Many of these features are also typical findings of IBD, leading clinicians to misdiagnose such cases.
In this case, the colonoscopic findings in our center suggested mild proctitis, but the findings were not consistent with the typical findings for IBD. Yet, the diagnosis was delayed because of the nonspecific clinical presentation of this case, the physicians' unawareness of chlamydial proctitis, and the lack of routine diagnostic tests for this disease.37 Because we did not have serovar-specific serologic tests for C. trachomatis available and the patient had neither genital ulcers nor lymphadenopathy, we empirically treated him with the recommended regimens for non-LGV proctitis.10 If perianal ulcers or mucosal ulcers of the rectum had been present on colonoscopy, treatment should have followed the regimens for LGV proctitis of doxycycline 100 mg orally twice daily for 3 weeks.
In conclusion, chlamydial proctitis may be confused clinically, endoscopically, and histologically with IBD. Clinicians should be sure to remember C. trachomatis infection as a cause of proctocolitis in men who are involved in homosexual activities and obtain a thorough sexual history in those with risk factors. We found several reported cases of chlamydial proctitis that had first been misdiagnosed as IBD in Western countries, but not in Korea. This may be due to the smaller number of people involved in homosexual activities in Korea compared with North America and Western Europe. However, as more people engage in homosexual activities and the prevalence of HIV increases in Korea, physicians must be aware of the proctitis caused by STDs and the resemblance to IBD. Prompt diagnosis is important because untreated disease can lead to significant complications including formation of granulomas, strictures, fistulas, and perirectal abscesses.9 Furthermore, the ulcerative nature of LGV may facilitate both transmission and acquisition of HIV and other STDs up to nine-fold.6 Therefore, identification of C. trachomatis infection is crucial for treatment of the disease and prevention of irreversible sequelae.

 XML Download
XML Download