

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stress urinary incontinence (SUI) is a complaint of involuntary leakage in situations of effort or exertion, or upon sneezing or coughing, and more than half of women with urge incontinence have SUI.1,2,3 Either autologous or synthetic material can be used to suspend the patient's urethra, which prevents the leakage of urine from the bladder. Although the Burch colposuspension has been considered the gold standard surgical procedure for the treatment of SUI, mid-urethral procedures such as tension-free vaginal tape (TVT) and transobturator tape (TOT) procedures are both commonly practiced and are successful techniques using synthetic material for urethral suspension.4 The cure rate of both techniques has been reported to range between 84% and 93%.5,6
Since TVT was introduced in 1996, it has been considered the treatment of choice for SUI. However, complications such as bladder perforation, hematoma, nerve injury, and major vessel or bowel injury led to the development of the TOT procedure.7,8,9,10,11,12 Although TOT has been reported to be a safe and cost-effective method, its success rate remains questionable.4,6,8,13,14,15 To improve the success rate of TOT procedures, our intraoperative test was performed before application and adjustment of the mesh to control the tension of the tape after observing the degree and pattern of urine leakage. We studied whether this method had an effect on the success rate of TOT procedures.
Go to : 
MATERIALS AND METHODS
The study was conducted on randomly selected patients who visited our hospital between January 2007 and May 2011. All patients had suffered from SUI and presented with an abdominal leakage pressure lower than 120 cmH2O in the urodynamic study and were treated with a TOT surgical procedure. Those who had other pelvic organ diseases such as prolapses were excluded. A total of 96 patients were included: 47 patients underwent a TOT procedure without the intraoperative provocative test from January 2007 to December 2009 (Group I), and 49 patients underwent a TOT procedure with the intraoperative provocative test from January 2010 to May 2011 (Group II).
The intraoperative test was conducted to observe the degree and pattern of the urine leakage before application and adjustment of the mesh by coughing or manual pressure on the suprapubic area. Bladder filling was performed with at least 300 ml of normal saline during the intraoperative test. After observing the degree and pattern of the urine leakage, we controlled and adjusted the tension of the mesh.
Preoperative and postoperative examinations of the uroflowmetry and residual urine were conducted for all patients. The success of the treatment was checked 3 months and 6 months after the surgery according to the Patient Global Impression of Improvement (PGI-I) scale. The SUI symptoms were the main criterion for the efficacy of the maneuver. The patients who required medication for urgency after the surgery were grouped as "improved," and those who did not were grouped as "cured." In the patient group that was defined as "improved," the patients who did not experience any effect from the medication and those who were unsatisfied were grouped as "failed."
Statistical analyses were performed by using SAS (version 9.2, SAS Inc., Cary, NC, USA). A t-test (Table 1), Fisher's exact test (Table 2), and a logistic regression analysis (Table 3) were used to identify the statistical differences between the two groups. In all the analyses, values of p<0.05 were considered to be statistically significant.
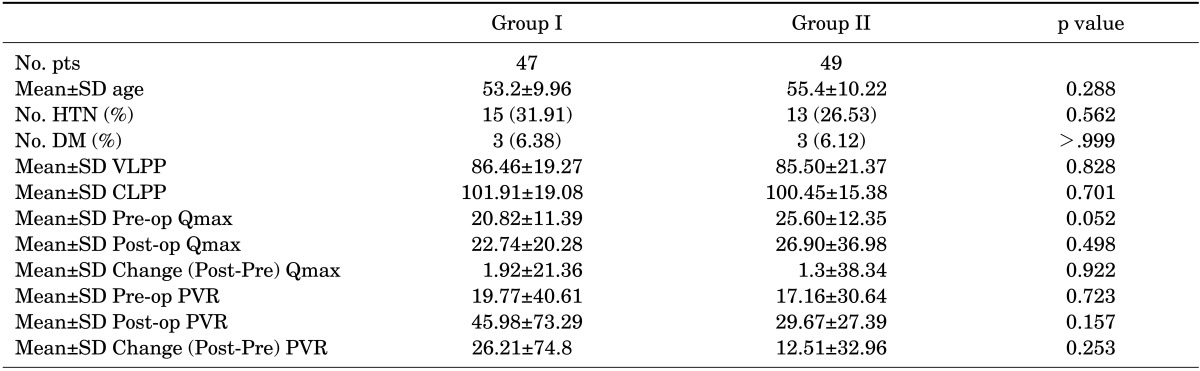
TABLE 1
Patient characteristics including VLPP, CLPP, Qmax, and PVR in Group I and Group II
SD: standard deviation, HTN: hypertension, DM: diabetes mellitus, VLPP: Valsalva leak-point pressure, CLPP: cough leak-point pressure, Qmax: peak flow velocity in the uroflowmetry, PVR: postvoiding residual volume, Change (Post-Pre) Qmax: change in values between postoperative and preoperative Qmax, Change (Post-Pre) PVR: change in values between postoperative and preoperative PVR.
![]()
Go to :
RESULTS
The patients were selected randomly in order to match the patient characteristics of the two groups. The average age in each group was 53.2 (±9.9) and 55.4 (±10.2) years.
The Valsalva leak-point pressure (VLPP) and cough leak-point pressure (CLPP) of Group I were 86.46 cmH2O and 101.91 cmH2O, respectively, and the corresponding values of Group II were 85.50 cmH2O and 100.45 cmH2O.
The preoperative and postoperative peak flow velocity (Qmax) measured by uroflowmetry of Group I were 20.82 ml/s and 22.74 ml/s, respectively, and the corresponding values of Group II were 25.60 ml/s and 26.90 ml/s. The postvoiding residual urine (PVR) before and after surgery was 19.77 ml and 45.98 ml in Group I and 17.16 ml and 29.67 ml in Group II, respectively. Changes in the postoperative and preoperative Qmax and PVR in Group I were 1.92 ml/s and 26.21 ml, respectively, and the corresponding values in Group II were 1.3 ml/s and 12.51 ml. The Qmax and PVR values in both groups indicated that the average values had increased after surgery. In particular, Group I showed a greater degree of variance in Qmax and PVR than did Group II, but both groups had large standard deviations and no statistically significant difference in the variances was found between the two groups (Table 1). A multivariable linear regression was not performed for the univariable analysis in Table 1 because a statistically significant difference did not exist in the variances of the Qmax and PVR between the two groups.
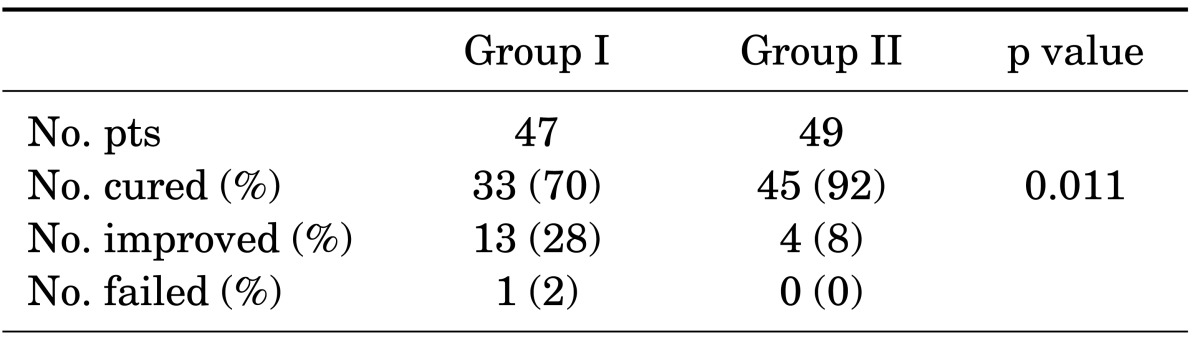
In Group I, the cure rate was 70.2%, the improved rate was 27.7%, and 1 patient showed no improvement after treatment. In Group II, the cure rate was 91.8%, the improved rate was 8.2%, and none of the patients failed to show improvement. Group II had a significantly higher success rate than did Group I (p=0.011; Table 2).
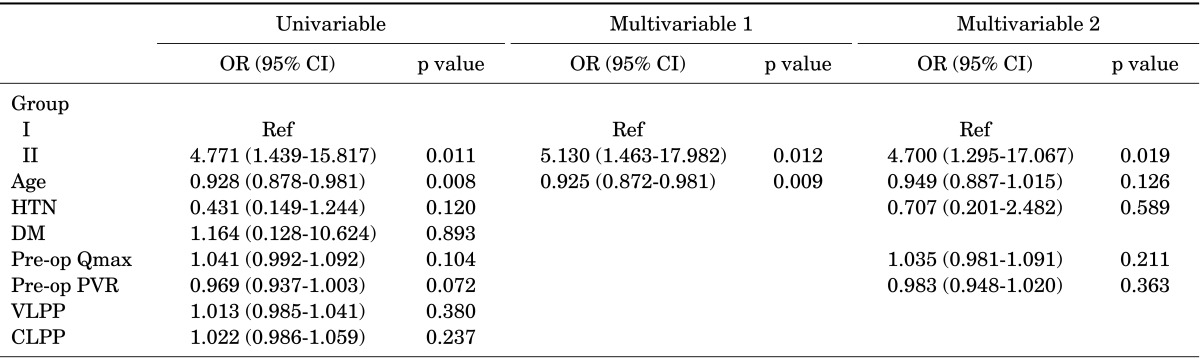
A logistic regression analysis was additionally performed because a statistically significant difference in the cure rate between the two groups existed. By using the incidence of being cured as a dependent variable, the clinically important variables were verified in a univariable logistic regression analysis. In the univariable logistic regression analysis between the two groups, Group II exhibited a higher odds ratio (OR: 4.771) than did Group I for the cure rate and Group II had a higher success rate than did Group I (p=0.011).
A multivariable logistic regression was performed, and age was calculated in the range of a p value<0.05 [OR: 0.928; 95% confidence interval (CI): 0.878-0.981; p=0.008] determined on the basis of the univariable logistic regression analysis. Differences between the two groups were identified (OR: 5.130; 95% CI: 1.463-17.982; p=0.012) and were considered statistically significant. To calculate further clinically important variables, age, hypertension, preoperative Qmax, and PVR in the range of a p value<0.15 were calculated, and differences between the two groups were identified (OR: 4.700; 95% CI: 1.295-17.067; p=0.019). The cure rate of Group II was verified to be significantly higher than that of Group I, and it was found to be statistically significant (p=0.019; Table 3).
Go to :
DISCUSSION
SUI is a common medical problem affecting 12.2% to 26.4% of women, and 50% of women with urinary incontinence have SUI.2,3 Epidemiologic studies conducted on the Korean population have reported that 24.4% to 40.8% of all Korean women have UI, and 48.8% to 72.8% of women with UI have SUI.16,17,18 Numerous treatment options for SUI are available. Conservative therapies such as pelvic floor muscle training, compression devices such as pessaries, and pharmacotherapies (i.e., duloxetine) can be offered before surgery.19 Many patients still require surgical treatment, and the gold standard for the treatment of SUI is the Burch colposuspension and autologous fascial sling.20 However, ever since Ulmesten and Petros introduced the tension-free vaginal tape, the midurethral sling has become the standard treatment for SUI.8 The TVT procedure has been widely adopted. Although the incidence is rare, severe complications such as perforation, hematoma, nerve injury, and major vessel or bowel injury can occur with the TVT procedure and have led to the development of the TOT procedure.7,8,9,10,11,12 Many studies comparing TOT and Burch surgery have reported that TOT is associated with a shorter operation time and length of hospital stay, and the surgical complications and cure rates are either similar or superior to those of the Burch operation.4,21 Although the TOT procedure has been reported to have lower risks of complications than the TVT procedure, it was reported to be equivalent or inferior to the TVT procedure in its effect.8,13,22,23,24,25
To our knowledge, this is the first report on the effect of an intraoperative provocative test before application of the mesh. When our intraoperative provocative test was used, the cure rate was 91.8%, which was significantly higher than the 70.2% when the provocative test was not used. Studies by other groups have used different methods to evaluate the cure rates, so direct comparison is not possible. However, our result is comparable to the 81% to 90.3% reported by other studies.4,6,22,23,24,25
Although a few studies have shown that the location of the tape and urethral compression by the tape affect the cure rate, there has not yet been a report on surgical methods to improve the success rate of sling procedures.26 Incomplete compression of the urethra can lead to recurrent urinary incontinence after the surgical treatment of SUI. This report shows that applying an intraoperative provocative test before applying the mesh is an effective method for preventing the operator from exerting incomplete tension or excessive tension while adjusting the tape. Excessive tension may lead to postoperative obstruction, although there were no patients with such results in the current study. Further study of the maneuver is needed, such as of the appropriate pressure to apply and of the methods to use to avoid exerting excessive tension on the tape. The advantage of our method is that the surgeon can guess the appropriate tension to apply and control the tension of the mesh after observing the degree and pattern of the urine leakage intraoperatively. However, our report has some limitations because the provocative test is not objective but subjective, and this was a retrospective study.
In conclusion, the TOT procedure is an effective procedure to treat SUI. However, its cure rates still need improvement. Inadequate tension of the tape can lead to incomplete compression of the urethra, leading to recurrent urinary incontinence after surgical treatment. Conversely, excessive tension of the mesh may lead to postoperative obstruction. Our method presents some advantages in that the surgeon can control and adjust the tension of the mesh after observing the degree and pattern of the urine leakage. Further study and refinement of the method are needed.
Go to :
 XML Download
XML Download