

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Percutaneous nephrolithotomy (PCNL) is an effective choice in the treatment of large kidney stones because of excellent outcomes and acceptably low morbidity, and it is usually performed with the patient in the prone position.1 This approach provides a larger surface area for the choice of puncture site and a wider space for instrument manipulation. However, the prone position has several disadvantages: respiratory and cardiovascular risks; ventilatory difficulties, especially in obese patients and in elderly patients with compromised cardiopulmonary status;2,3 and the need for position changes during the procedure. For these reasons, many urologists have tried modified positions for PCNL (flank, supine, and modified supine).4,5
Supine PCNL was first reported by Valdivia Uría et al. in 19983 and is regarded as possessing several advantages. Anesthesiologists prefer the supine position because of better airway control during procedures. Another advantage of the supine position is that there is no need for position changes to perform other endoscopic procedures such as cystoscopic or ureteroscopic operations.6 The supine position enables simultaneous retrograde ureteroscopic procedures during PCNL without any position change. A nephrostomy catheter has routinely been placed after PCNL, because it provides proper drainage of urine, prevents urinary extravasation, and enables tamponade of bleeding.7,8 The need for placement of a nephrostomy catheter has been questioned, however, owing to increases in postoperative discomfort and morbidity, and several studies in the past two decades have demonstrated the feasibility of tubeless PCNL. In the current study, we evaluated the feasibility and efficacy of intermediate-supine PCNL in our initial experiences with this approach.
Go to : 
MATERIALS AND METHODS
1. Patients
The study was approved by the institutional review board of our institution. Between January 2012 and October 2012, a total of 15 patients with renal stones underwent PCNL in the intermediate-supine position performed by a single surgeon (K.S.C.). Preoperative data, operative outcomes, and postoperative outcomes were retrospectively collected and evaluated.
2. Operative procedures
Before surgery, the desired calyx was punctured under fluoroscopy guidance and a guidewire was inserted by an interventional radiologist. Then a PCNL was performed with the patient under general anesthesia in the intermediate-supine position. For intermediate-supine PCNL, the patient was placed in the supine position with a 1-L saline bag below the ipsilateral flank. Thus, the ipsilateral flank was elevated 20°, causing the posterior calyx to project more laterally (Fig. 1). In a selected patient, a retrograde ureteral occlusion catheter was fixed through the ipsilateral ureteral orifice by use of cystoscopy. Under the guidance of C-arm fluoroscopy, we accurately assessed the punctured calyx through a guidewire placed in the intervention port. The tract was dilated by using a 30-Fr balloon dilator. After Amplatz sheath insertion, the nephroscope was introduced, and the stones were fragmented by using a LithoClast™ lithotripter (Electro-Medical Systems, Nyon, Switzerland) and were extracted by use of stone forceps or a suction catheter. After completion of stone removal, antegrade placement of a double-J ureteral stent was performed in most cases. A nephrostomy tube was used when needed according to the surgeon's decision. If there was no significant bleeding and no significant injury to the renal pelvis or ureter, a tubeless PCNL was performed.
 | FIG. 1Intermediate supine and tubeless percutaneous nephrolithotomy. (A) The position was modified using a one liter saline bag below the ipsilateral upper flank in a male patient. (B) Renal stones were removed using LithoClast by the operator and assistant who were seated during the procedure. (C) There was no nephrostomy catheter placed in the puncture site in a female patient after operation.
|
3. Outcome measures and statistics
In all cases, the stone size was measured with noncontrast computed tomography (CT) and was calculated by use of the following formula: width×length×π×0.25.9 Complete stone-free status was defined as no stone fragments visible on the postoperative image study, and the operation was considered successful if the patient had either no or clinically insignificant residual stone fragments (largest stone diameter less than 4 mm and asymptomatic, nonobstructive, and noninfectious).10,11
Length of hospital stay was defined as the time interval between the day of surgery and the day of discharge from the hospital. Perioperative complications were evaluated according to the Dindo-modified Clavien system validated in 2004.12 Pain was evaluated every 8 hours by a trained nurse using the visual analogue scale (VAS) for pain. Patients with moderate to severe pain were given tramadol 50 mg intravenous (IV) or pethidine 25 mg intramuscular (IM) if postoperative pain was not controlled with nonsteroidal analgesics. All patients were monitored for levels of hemoglobin and serum creatinine preoperatively and by the seventh postoperative day. A plain x-ray or an abdomen-pelvis CT was obtained within 1 to 3 months postoperatively. The patient was discharged when he or she was thought to be free of complications and when the patient's pain was controlled with oral analgesics (VAS pain score lower than 3). The preoperative and postoperative VAS pain scores and serum creatinine variations among the subjects were analyzed by use of the Wilcoxon signed rank test. Comparisons with a p-value less than 0.050 were considered to be statistically significant. Data analysis was performed by using PASW (version 18.0; SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
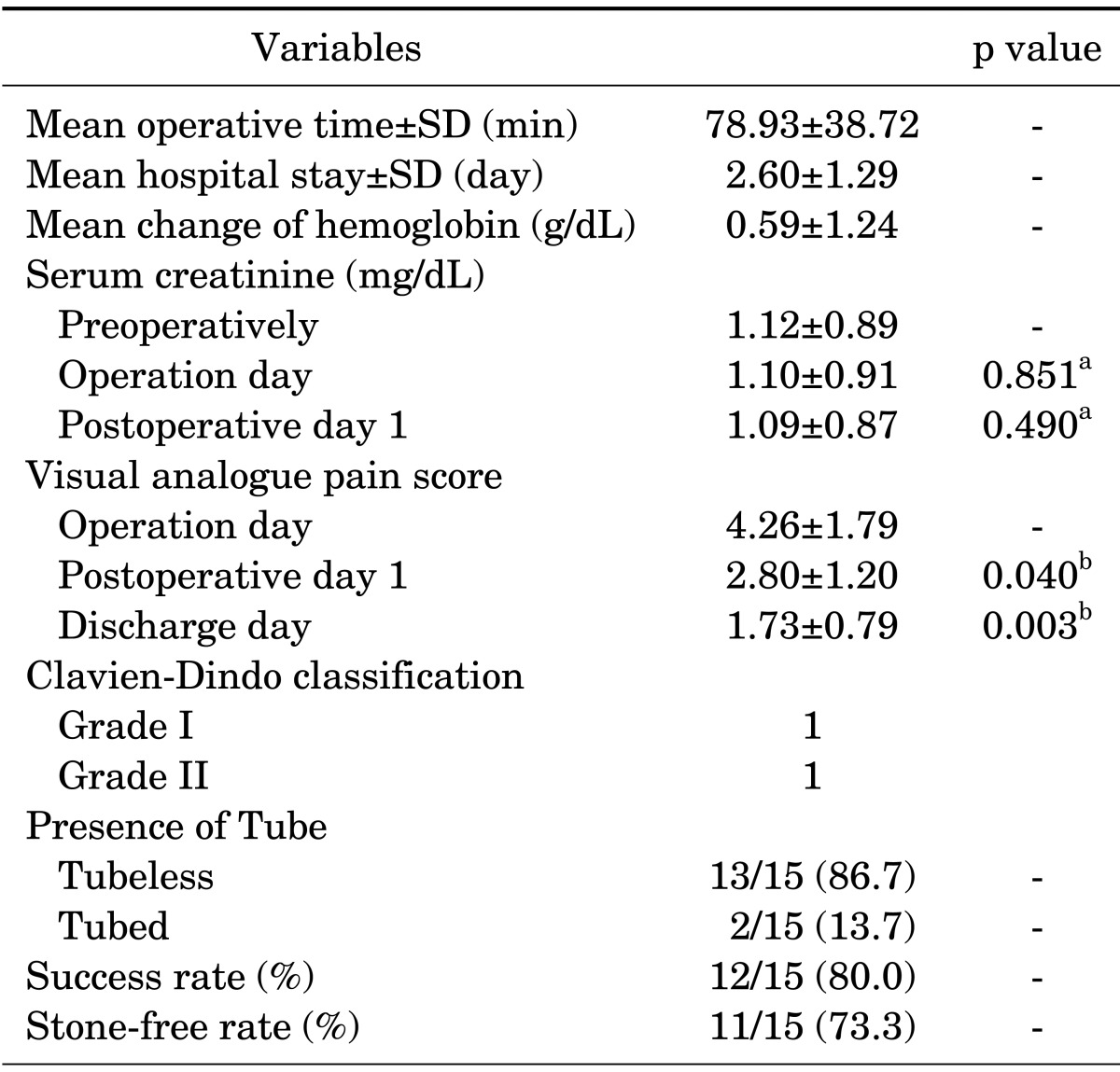
We performed a total of 15 PCNL procedures with patients in the intermediate-supine position (Table 1). The mean patient age was 58.77±17.33 years, and the patients' mean body mass index was 26.17±4.22 kg/m2. The mean renal stone size was 5.48±5.69 cm2. The average operative time was 78.93±38.72 minutes (Table 2). The average hospital treatment stay was 2.60±1.29 days. A nephrostomy catheter was inserted in two cases (13.3%); significant venous bleeding was suspected in one case, and a second-look operation was considered in one case. In 13 cases (86.7%), intermediate-supine PCNL was completed without nephrostomy tube placement. An antegrade ureteral stent indwelling at the ipsilateral site was performed in 14 cases. In two patients, the retrograde procedures were simultaneously performed without a change in position (one ureteroscopic ureterolithotomy and one transurethral placement of an occlusion catheter).
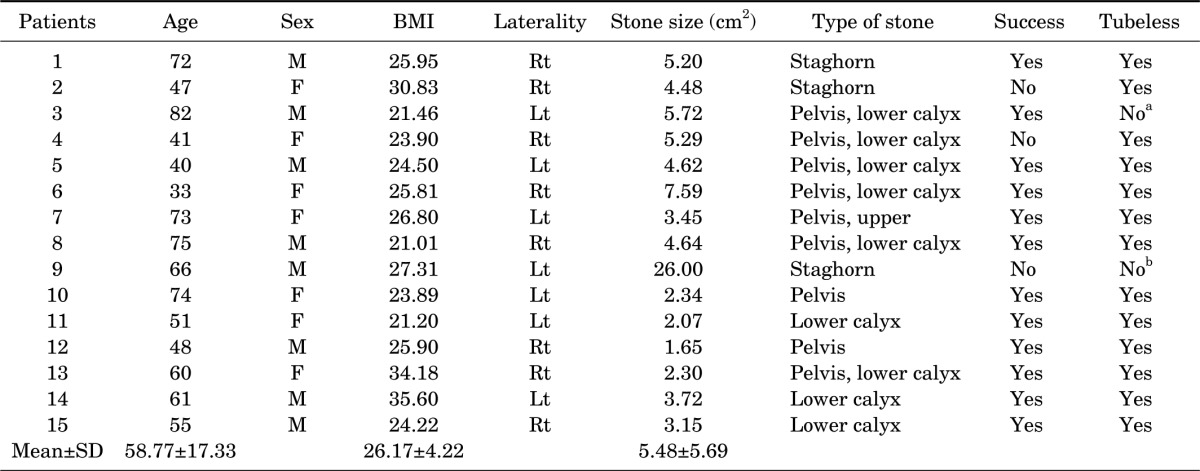
The success rate was 80.0%, and the complete stone-free rate was 73.3%. Three patients with a significant remnant stone were also successfully managed with additional procedures. One patient underwent a second-look operation owing to a large stone burden (26.00 cm2) and long operative time (191 min) at the first operation. In the other two patients, it was anatomically difficult to obtain proper access to the remnant stones, which were relatively small, and the stones were successfully treated with shock wave lithotripsy.
Only two patients had mild complications according to the Clavien-Dindo classification (Grade I in one patient and Grade II in one patient). Transfusion was needed in only one patient (6.7%).
The average variation between preoperative and postoperative hemoglobin was 0.59±1.24 g/dL. Serum creatinine levels measured preoperatively, on the day of surgery, and on postoperative day one were 1.12±0.89 mg/dL, 1.10±0.91 mg/dL (vs. preoperatively; p=0.851), and 1.09±0.87 mg/dL (vs. preoperatively; p=0.490), respectively. Generally, pain was tolerable within 2 to 3 days; the VAS scores for pain on the day of surgery, on postoperative day one, and on the day of discharge were 4.26±1.79 (vs. operative day; p=0.040), 2.80±1.20, and 1.73±0.79 (vs. operative day; p=0.003), respectively.
Go to :
DISCUSSION
Many urologists have attempted to overcome the disadvantages of conventional PCNL, and the technique of PCNL has largely evolved in terms of the placement of tubes and changes in position over the past two decades. Many cases of both supine PCNL and tubeless PCNL have been accumulated, but data are lacking for supine PCNL in conjunction with the tubeless technique. Our early experiences suggested that intermediate-supine and tubeless PCNL is a safe and effective choice that offers several advantages with excellent outcomes. These experiences are consistent with a previous report by Rana et al.13 Those authors maintained that PCNL with the patient in the supine position has several advantages, such as a lower rate of complications, a shorter operative time, and the simplicity and ease of performance of the procedure. Therefore, the procedure can provide uniform comfort for the anesthesiologist, patient, and surgical team.
When the PCNL procedure is performed with the patient in the prone position, a ureteral catheter is commonly fixed in the lithotomy position before the patient is turned; however, PCNL in the supine position does not require turning. Furthermore, PCNL in the intermediate-supine position facilitates the completion of ureteroscopic processes at the same time. Therefore, the operative time for PCNL in the supine position is shorter than that for PCNL in the prone position.14 PCNL with the patient in the supine position saves 30 to 40 minutes of operative time and avoids the risk associated with a position change under general endotracheal anesthesia. Actually, many recent studies have reported shortened operative times. De Sio et al.14 reported that the operative time was 68 minutes (range, 55-140 minutes) in the prone position but 43 minutes (range, 25-120 minutes) in the supine position (p<0.001), and Karami et al.15 reported that the operative time was reduced in the lateral position (74.4±26.9 minutes), prone position (68.7±37.4 minutes), and supine position (54.2±25.1 minutes) (p<0.040).
Many studies have reported high success rates of supine PCNL. De Sio et al.14 reported that in their randomized controlled study, the stone-free rate was excellent in both the supine (88.7%) and the prone (91.6%) position PCNL groups. Shoma et al.16 reported similar success rates for the supine (89%) and prone (84%) positions in a prospective nonrandomized study, and Karami et al.15 reported that the success rate was 92% in the prone position, 86% in the supine position, and 88% in the lateral position.
The success rate of supine PCNL is also dependent on the stone size and location. Hoznek et al.17 demonstrated that the success rate was 90% for single stones, 78% for multiple stones, and 43% for staghorn stones during supine PCNL. Xu et al.18 also suggested similar stone-free rates of 85.7% overall, 92.2% for a single calculus, and 72.9% for staghorn calculi.
In the supine and intermediate-supine positions, mobile fluoroscopy (C-arm) can be utilized without the interrupted artifacts (spine, ribs, etc.) that are present in the lateral position, which might be helpful in improving surgical outcomes such as the stone-free rate.16,19 On the contrary, there are some limitations in using fluoroscopic examination during PCNL in the lateral position because of the possibility of the aforementioned artifacts.
For the PCNL procedure, several studies have reported that the rate of significant bleeding requiring transfusion was about 1.5% to 9%3,13,16,19 and was directly related to the stone size, procedure time, and creation of multiple tracts.20 Basiri and Mohammadi Sichani21 suggested that the risk of bleeding might be less in the supine position than in the prone position because a backflow of blood to the renal vein is caused by obstruction of the inferior vena cava. Also, there might be less risk of colonic injury during supine PCNL because of the more anterior displacement of the colon away from kidney in the supine position than in the prone position.3,22 Valdivia Uría et al.3 reported no damage to the peritoneum and colon in a CT study and confirmed that the colon was further away from the kidney in the supine position than in the prone position. In their report on 557 patients, the operation was successful in 93% of the cases, with a low complication rate and no colonic perforation.3 However, a different study reported similar colonic injury risk between the supine position and the prone position.18 Meanwhile, severe anesthesia complications are rarely reported in the prone position, and it is generally accepted that the supine position is more satisfactory for the anesthetist, especially in obese or high-risk anesthesia patients.23 In the prone position, it is difficult for the anesthetist to observe the patient effectively, and the prone position may not be favorable for resuscitation when acute syndromes such as obstruction of respiratory passages or acute myocardial ischemia occur during the operation.24
Nevertheless, PCNL in the supine position also has several disadvantages. Because the angle between the surface of the operation table and the anterior calyxes is smaller than that in prone position, it is difficult to access stones in the anterior calyxes.14,16,21 Approaching the upper calyx is more difficult in the supine position, especially if placed overly medially, and this problem is more obvious on the left side.13,21 Another disadvantage in the supine position is the mobility of the kidneys, which is greater than in the prone position. Therefore, the kidneys are easy to move anteromedially during tract formation in the supine position. Finally, the pyelocaliceal system is constantly collapsed in this position; thus, nephroscopic procedures might be more difficult.19
Although there have been some debates on the efficacy and safety of tubeless PCNL, successful experiences by many urologists have rekindled clinical interest in tubeless or totally tubeless PCNL. According to recent studies, there is no significant difference in the rate of complications between standard PCNL and tubeless PCNL, and tubeless PCNL has several advantages.25,26 Tubeless PCNL is associated with a shorter length of hospital stay; thus, patients can return quickly to everyday life, experience less pain, and incur a lower cost. Multiple studies have found these data to be statistically significant. Sofikerim et al.27 reported that tubeless PCNL is a safe and effective technique even after supracostal access and is associated with less postoperative pain and a shorter hospital stay. Shen et al.28 suggested that the hospital stay of the tubeless group was less than that of the middle-tube and large-tube groups in a multiple center metaanalysis. They recommended that a nephrostomy catheter be placed in certain situations (multiple access, major damage to the collecting system, possibility of a second look operation, severe intraoperative bleeding, complicated cases, and intrathoracic trauma).29 The disadvantages of the tubeless procedure, including the need to place a ureteral stent, should be considered; patients may have bladder irritation symptoms such as flank pain, gross hematuria, urinary frequency, and urgency because of the placement of a ureteral catheter, and patients must undergo cystoscopy to remove the ureteral stent.30
There were several limitations to our study. It was a retrospective and noncomparative analysis confined to small numbers of early experiences. In addition, we did not attempt multiple accesses or an upper pole approach, and we selected relatively simple cases, although there were also some difficult cases with large staghorn stones among our early experiences. Nevertheless, intermediate-supine and tubeless PCNL might be a safe and effective option that offers several advantages with excellent outcomes in the management of renal calculi. Thus, a prospective randomized study with a larger population is needed to confirm our observations.
In conclusion, intermediate-supine PCNL is believed to be feasible and effective and is associated with several advantages. It may shorten the preparation period of the operation and the operative time, and it can result in a high stone-free rate with low complications. In our series, there was no increase in the bleeding risk with the intermediate-supine position; therefore, the tubeless technique could be applied in most cases. The tubeless technique also seems to have contributed to the favorable surgical outcomes in our early experiences. A prospective randomized study with a larger population is needed to verify our outcomes.
Go to :
 XML Download
XML Download