

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acinetobacter species are aerobic gram-negative bacilli that are ubiquitous in natural environments such as soil and water. These species are occasionally found as commensals on the skin and throat and in secretions of healthy people. It was previously believed that Acinetobacter species were not a common human pathogen and that they were uncommon causes of infection. However, Acinetobacter species are now one of the most common organisms isolated from hospital environments and hospitalized patients.1
Acinetobacter species have excellent biofilm-producing ability and intrinsic and acquired resistance to various antibiotic agents, all of which facilitate their survival in hospital environments. For these reasons, Acinetobacter species are frequently found on the skin and in the respiratory and urinary tracts of hospitalized patients.
MICROBIOLOGY AND TAXONOMY
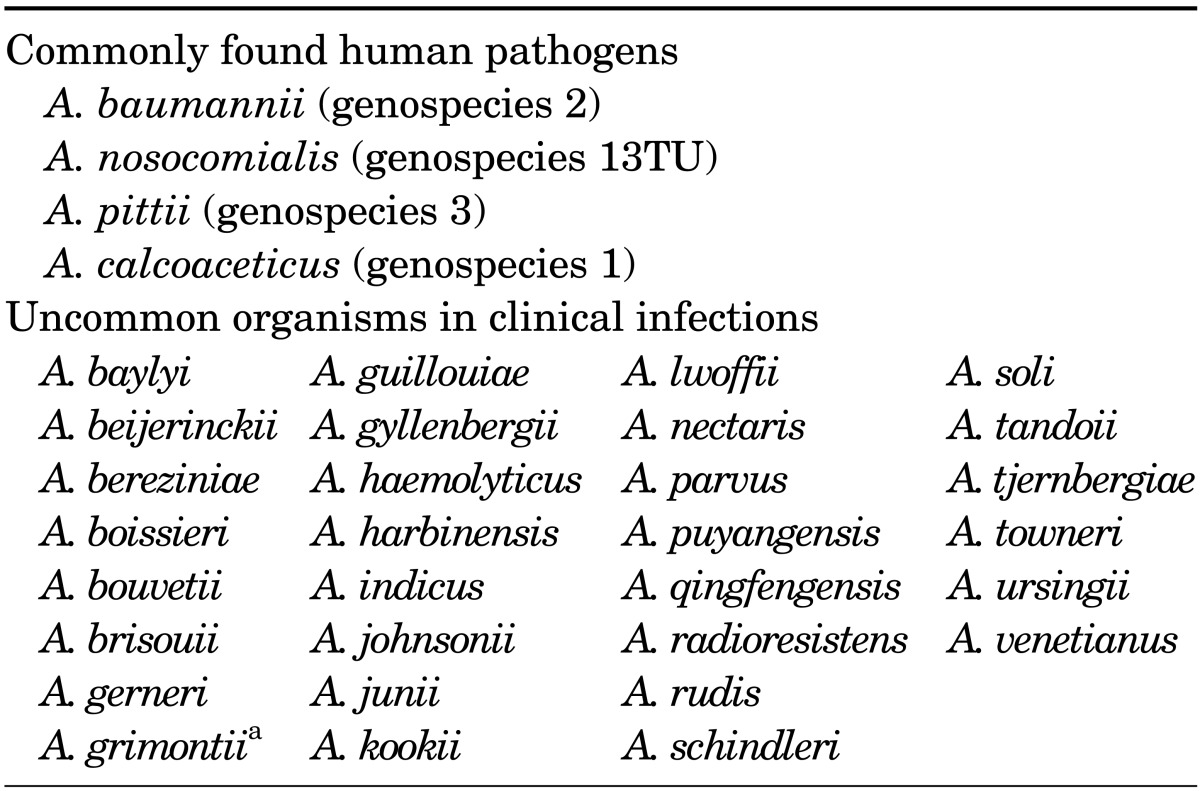
The genus Acinetobacter belongs to the subclass γ-Proteobacteria, family Moraxellaceae, and comprises a heterogeneous group of aerobic nonhemolytic gram-negative coccobacilli, which are usually found in diploid formation or chains of variable length. Acinetobacter spp. are oxidase-negative, catalase-positive, indole-negative, and nitrate-negative. However, identification of individual species by their phenotypic traits is difficult, and identification of individual species by use of current automated or manual commercial systems will require further confirmation testing. Nowadays, with advancements in molecular bacterial taxonomy, particularly 16S rDNA sequencing and DNA-DNA hybridization, species can be distinguished more accurately. Currently, the genus Acinetobacter contains 34 formally named species (Table 1).2
Among the Acinetobacter species, Acinetobacter baumannii, Acinetobacter pittii (genospecies 3), and Acinetobacter nosocomialis (genospecies 13TU) (together forming the "A. baumannii complex") are closely related; they are considered important nosocomial pathogens and account for most clinically significant infections. These three species together with another closely related Acinetobacter species commonly found in the natural environment, Acinetobacter calcoaceticus, are grouped under the term "A. calcoaceticus-A. baumannii complex" (ACB complex).
PATHOGENESIS
Acinetobacter was initially considered to be an organism of low virulence, and little is known about its virulence mechanisms and host responses. Several specific potential virulence mechanisms related to the ability of Acinetobacter species to adhere to, colonize, and invade human epithelial cells have been identified. However, despite recent advances, many questions regarding the virulence and pathogenesis of Acinetobacter species remain unanswered.
The pathogenic determinants include pilus-mediated biofilm formation,3 an outer membrane protein A associated with apoptosis in human cells,4,5 an iron-acquisition system,5,6 lipopolysaccharides,7 and a quorum-sensing system.8 Biofilm formation can be considered a key virulence factor of many A. baumannii isolates, including carbapenem-resistant strains. A biofilm constitutes living bacteria attached to a surface as sessile communities,9 which enables bacteria to withstand host immune defense mechanisms, antibiotics, and hydrodynamic shear forces. This allows A. baumannii to colonize and persist on biotic and abiotic surfaces, causing infections associated with indwelling medical devices. Recent studies have shown that ACB complex species are threefold more likely to form a biofilm at a liquid-solid interface than are non-ACB complexes at 25℃ (80-91% versus 5-24%).10
RESISTANCE MECHANISMS
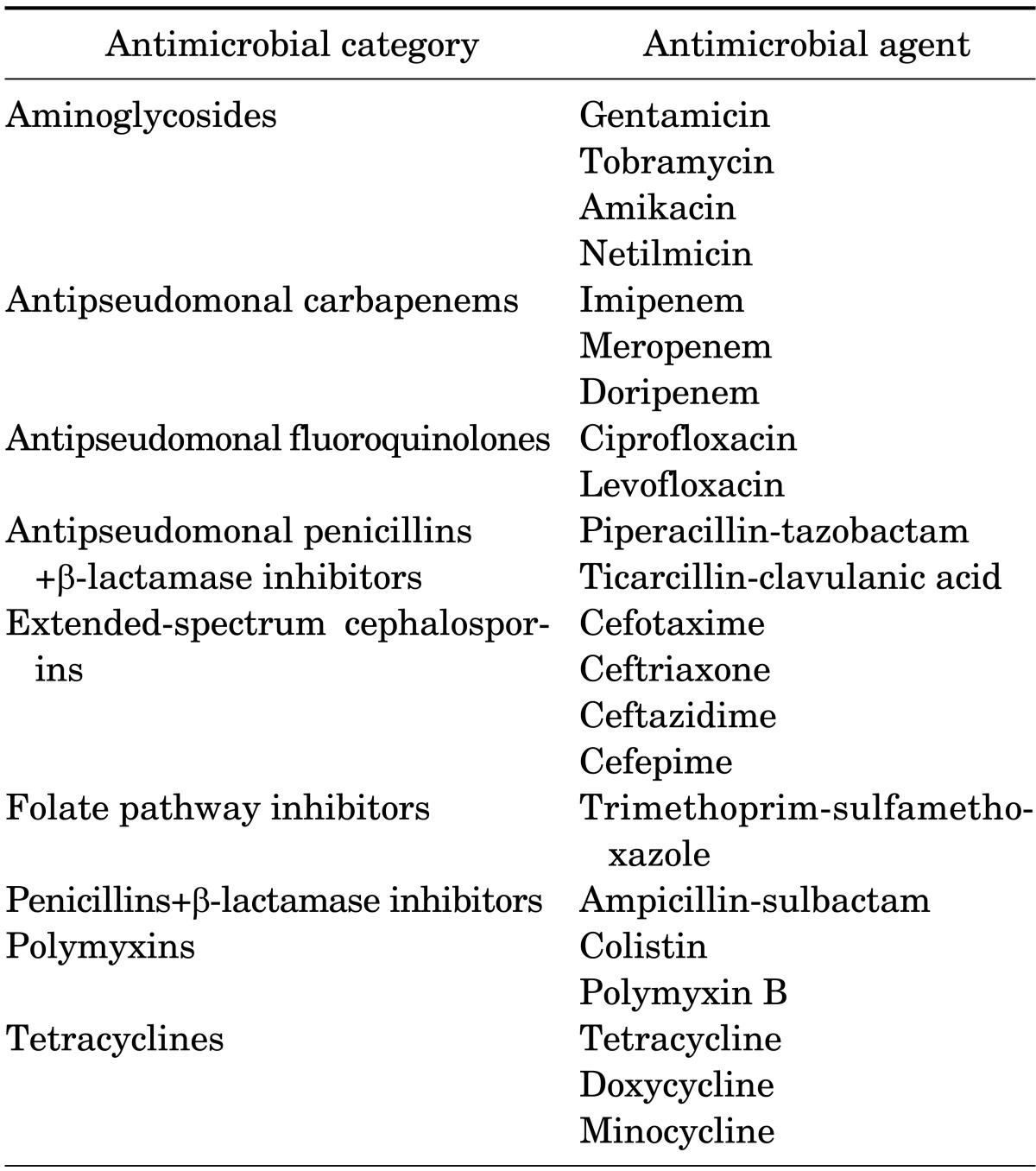
Acinetobacter species are a common cause of nosocomial infections, and some Acinetobacter isolates are resistant to all or almost all β-lactam antibiotics, aminoglycosides, and quinolones. However, controversy exists over the terms "multidrug resistance" (MDR), "extreme drug resistance" (XDR), and "pandrug resistance" (PDR) in gram-negative pathogens, and a consensus on their definitions is needed. The most recent recommended updated definitions are as follows:11 MDR refers to a pathogen being nonsusceptible to at least one agent in more than three antimicrobial categories. XDR refers to a pathogen being nonsusceptible to at least one agent in all but less than two categories. PDR refers to a pathogen being nonsusceptible to all antimicrobial agents (Table 2).
Resistance mechanisms include inherent antibiotic resistance, antimicrobial-degrading enzymes, efflux pumps, target modification, and porin deficiency. The most important mechanism, however, is the endless capacity of Acinetobacter species to acquire antibiotic resistance, leading to MDR and even PDR.12 There are many mechanisms of antibiotic resistance; here we discuss only resistance to carbapenem and colistin.
Resistance to carbapenems is often mediated by serine oxacillinases (OXAs; Amber class D), which are encoded by the blaOXA-23, blaOXA-40, blaOXA-58, and metallo-β-lactamases (MBLs; Amber class B) genes of the VIM, IMP, and SIM families.13,14 OXAs are not inhibited by clavulanic acid and have been found in most regions of the world, whereas MBLs mediate resistance to carbapenems and all other β-lactamases, with the exception of aztreonam.14,15 Carbapenem resistance in A. baumannii isolates is most frequently due to OXA production, whereas MBL production is more prevalent in non-baumannii Acinetobacter isolates.13,16 In A. baumannii, the level of carbapenem resistance provided by OXAs is considerably lower than that mediated by MBLs. In particular, some of these enzymes do not hydrolyze meropenem.
The Acinetobacter mechanism of resistance to colistin differs from the usual mechanism in gram-negative pathogens,17 and investigations of these additional regulatory factors are ongoing. Currently, two main hypotheses regarding the resistance mechanisms exist. The first is the loss of lipopolysaccharide,18 and the second is a mutation in the genes encoding the PmrA and B proteins, which are related to increased expression of the PmrAB system and amino acid sequence alterations.19 Although acquired colistin resistance remains rare among clinical Acinetobacter isolates,20 some Acinetobacter species seem to possess intrinsic resistance to colistin without multidrug resistance.21 The emergence of colistin resistance has provided a safe and accurate method of determining the susceptibility of Acinetobacter species in a clinical setting. A comparison of the Vitek 2, MicroScan, and Etest methods with the agar dilution method for assessment of colistin susceptibility22 revealed that MicroScan was unreliable, whereas Etest and Vitek 2 were suitable for identification of colistin-resistant and colistin-susceptible Acinetobacter isolates.
EPIDEMIOLOGY
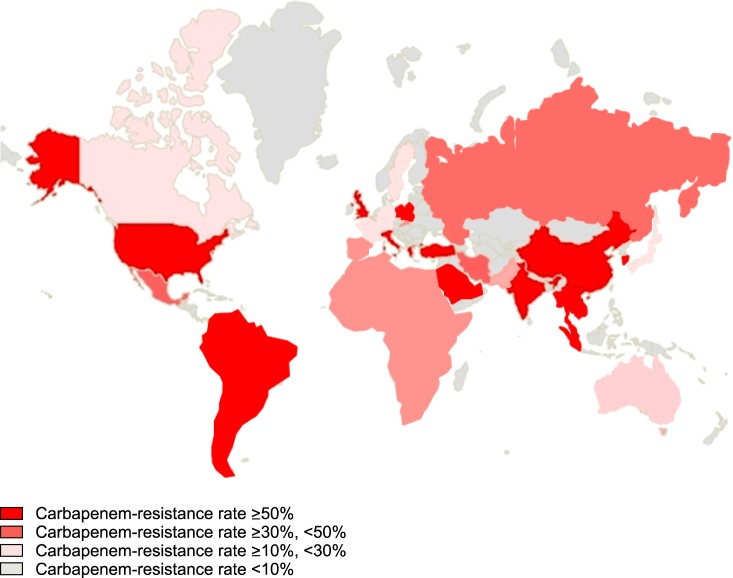
Carbapenemases have been reported increasingly frequently in Enterobacteriaceae and Acinetobacter species over the past 10 years worldwide (Fig. 1). The incidence of infections caused by carbapenem-resistant gram-negative bacilli in intensive care units (ICUs) has also increased; this now represents a global problem. Nosocomial outbreaks and endemic infections in ICUs are now commonplace because of the widespread use of broad-spectrum antibiotics and medical devices as well as an increase in the number of immunocompromised hosts.
Acinetobacter species comprise 8.4% of ventilator-associated pneumonia and 2.2% of central-line-associated bloodstream infections in the USA. Carbapenem resistance accounts for 65% of A. baumannii pneumonia in the USA and Europe,23 and clonal complex 92 was the most frequently identified worldwide.24 A recent study showed that >60% of A. baumannii isolates causing hospital-acquired pneumonia in Asian countries were PDR and carbapenem-resistant. Clonal complex 92, corresponding to global clone 2, was most prevalent, and OXA-23 oxacillinase was responsible for the majority of carbapenem resistance in the USA and Europe.25
CLINICAL FEATURES
Acinetobacter species have become a key concern owing to their ability to cause epidemics and nosocomial infections. Because of mechanisms that facilitate colonization of patients or devices used in hospital settings, Acinetobacter catheter or device-related infections are clinically important. A. baumannii is increasingly frequently responsible for nosocomial pneumonia in ICUs, predominantly ventilator-associated pneumonia, the incidence of which has increased from 4% (1986) to 7% (2003).26 Bloodstream infections due to A. baumannii account for 1% to 2% of all nosocomial bloodstream infections.27,28
A. baumannii is also a cause of urinary tract infections, commonly in patients with urinary tract catheters; surgical-site infections; and nosocomial meningitis.26
TREATMENT OPTIONS
Most A. baumannii strains are resistant to antibiotics such as penicillin, ampicillin, macrolides and second- and third-generation cephalosporins, ciprofloxacin, and chloramphenicol. Infections caused by antibiotic-susceptible Acinetobacter strains can be treated with ceftazidime, carbapenems, sulbactam, piperacillin/tazobactam, aminoglycosides, and quinolones (e.g., levofloxacin/ciprofloxacin) or cefepime, alone or in combination. Single-drug therapies with aminoglycosides are generally not recommended because of the high failure rates in Pseudomonas aeruginosa infections.29 However, the proportion of Acinetobacter infections caused by resistant strains is increasing and outbreaks of strains with PDR have been reported.30 The rate of Acinetobacter resistance to aminoglycosides and piperacillin/tazobactam is higher in Asian and European countries than in the USA.31
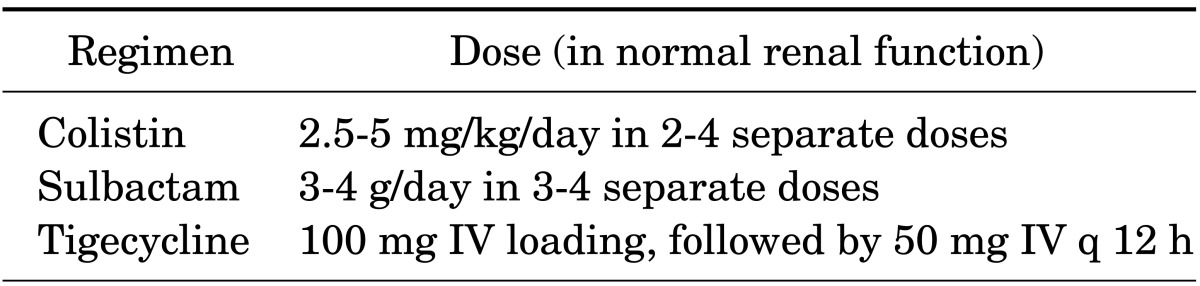
A number of studies have reported promising results regarding the efficacy of sulbactam against A. baumannii infections; indeed, in cases of sulbactam-susceptible A. baumannii, sulbactam was the preferred treatment option.32,33 For carbapenem-resistant Acinetobacter baumannii (CRAB) infections, sulbactam is more effective than polymyxins.34 Most studies prescribed 8 to 9 g of sulbactam per day in several doses, assuming normal renal function.34,35 Sulbactam is usually manufactured as a compound with ampicillin at a fixed ratio of 2:1. Although sulbactam appears to be effective against CRAB infections, an increasing number of sulbactam-resistant A. baumannii strains have been isolated; a recent study from Taiwan reported that 70% of clinical isolates were resistant to sulbactam.36
Another treatment option for CRAB infections is the polymyxins. Among them, polymyxins B and E (colistin) are suitable for clinical use and additional studies have been conducted on colistin and polymyxin B. Colistin can be injected into the bloodstream, ventricles, and spinal cord or can be administered as an inhalant. Owing to its renal toxicity, polymyxin had been one of the least-used antibiotics in practice. However, recently, the emergence of MDR in gram-negative bacteria has resulted in an increase in their use. Use of polymyxins for A. baumannii infections is clinically useful; however, a total cumulative dose of colistin appears to be associated with nephrotoxicity.37 Therefore, in patients requiring prolonged treatment, possible renal damage should be considered. Pharmacokinetic data on colistin are scarce and no consensus on the optimum method of its administration has been reached. The usual recommended dose for adults with normal renal function is 2.5 to 5 mg/kg/day as an intravenous colistin base in two to four doses (Table 3). However, a recent study suggested that a high dose with an extended-interval regimen can achieve better results.38 Because colistin has difficulty penetrating the blood-brain barrier, intra-ventricular administration of colistin is recommended for CRAB infections and Acinetobacter meningitis, as well during the removal of infected hardware.39,40
Colistin-based combination therapies in patients with CRAB infections remain controversial. In a randomized controlled clinical trial, a significant increase in the microbiological eradication rate was seen for a colistin and rifampicin combination, compared with colistin monotherapy, in serious XDR A. baumannii infections. However, 30-day mortality was not reduced by the addition of rifampicin to colistin.41 In another randomized trial, a colistin/fosfomycin combination exhibited a significantly enhanced microbiological response compared to colistin alone. However, although the clinical outcomes and mortality rates were lower in the combination therapy group, the difference was not statistically significant.42 In a prospective observational study, combination therapy was not associated with a reduced mortality rate in MDR A. baumannii infections.43 A recent meta-analysis indicated that various colistin-based combination therapy regimens showed no evidence of a benefit compared with monotherapies in the treatment of infections with carbapenem-resistant gram-negative bacteria.44
Tigecycline, which has shown in vitro activity against Acinetobacter species in skin and soft tissue infections45 as well as in complicated intra-abdominal infections,46 could be used as alternative therapy for CRAB infections. However, the use of tigecycline in patients with CRAB infections is limited, because the two major clinical CRAB infections are hospital-acquired pneumonia and central- catheter-related bloodstream infections. Tigecycline has been associated with an increased risk of mortality compared with other agents, most markedly among patients with hospital-acquired pneumonia.47 Moreover, tigecycline rapidly enters the tissues following administration, which results in low serum levels, making it inappropriate for the treatment of Acinetobacter bacteremia.48
A recent study found that aspergillomarasmine A, a natural fungal product purified from Aspergillus versicolor, was a rapid and potent inhibitor of carapenemase, including NDM and VIM, and fully restored the activity of meropenem against Enterobacteriaceae, Acinetobacter spp., and Pseudomonas spp. possessing either VIM or NDM-type alleles both in vitro and in mice.49 Further research is essential to evaluate the clinical efficacy, safety, and usefulness of this product and its derivatives.
OUTCOMES
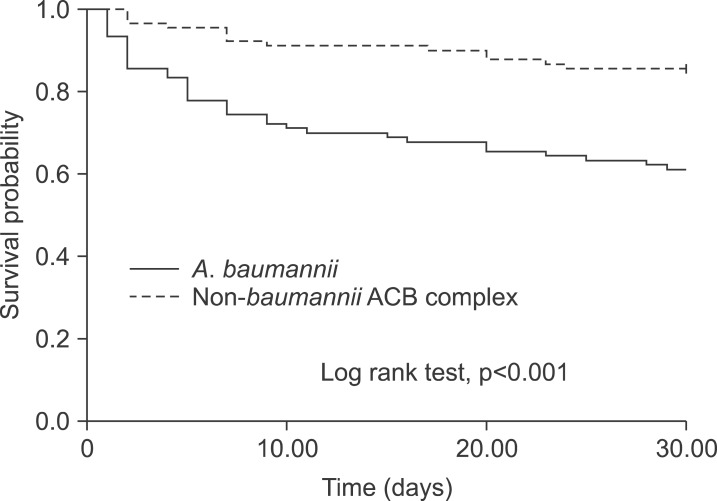
As mentioned previously, the ACB complex accounts for most nosocomial infections. Owing to its critical role in nosocomial infections and high mortality rates, much effort has focused on identifying the factors associated with the outcomes of Acinetobacter species infections. Several factors have been reported to influence the outcomes of Acinetobacter infections, including species differences, antibiotic resistance, and use of inappropriate empirical therapies. Although carbapenem resistance of other non-A. baumannii species has been documented, carbapenem resistance occurs most frequently in A. baumannii.50 This makes determination of the factors directly related to outcomes problematic. In an American study of 295 bloodstream infections caused by Acinetobacter species, the crude mortality rate of A. baumannii was higher than those of A. pittii and A. nosocomialis (36.9%, 13.0%, and 16.4%, respectively).51 Another study in Taiwan reported that bacteremia due to MDR stains appeared to be associated with a poor outcome, rather than A. baumannii itself.52 In our previous study, A. baumannii species, rather than antibiotic resistance, was found to be associated with mortality (Fig. 2).53 A study using a Galleria mellonella animal model reported that larvae survival was higher during infection with a non-baumannii ACB complex strain than with carbapenem-susceptible and carbapenem-resistant A. baumannii strains without appropriate treatment. No significant difference in survival was observed between larvae infected with carbapenem-susceptible and carbapenem-resistant A. baumannii.54 These data suggest that the factors contributing to the outcomes of Acinetobacter infections are more likely associated with differences in the virulence of individual species rather than carbapenem resistance. However, further investigation of the innate virulence of the various genospecies, and how these findings could be implemented in daily practice, should be carried out. Patients infected with A. baumannii had a mortality rate >30%. The poor outcome emphasizes the importance of aggressive infection control for prevention of mortality and the urgent need for new therapeutic agents and vaccines.
INFECTION CONTROL AND PREVENTION
Acinetobacter species are increasingly present in healthcare settings, either as occasional outbreaks or as endemic pathogens. Successful control has been reported in many healthcare facilities.55,56,57,58,59,60,61 However, once Acinetobacter has become endemic, it becomes difficult to eradicate from a healthcare facility. For this reason, early recognition, aggressive control of spread, and prevention of the establishment of endemic strains are crucial. Strategies for control of Acinetobacter outbreaks include active surveillance cultures, environmental surveillance cultures, improved hand hygiene, cleaning and disinfection of the environment, cohort nursing, isolation of patients in single rooms, restriction of access to the ICU, appropriate antibiotic use, and closing wards for cleaning and disinfection.62
MDR A. baumannii contamination of gloves, gowns, and hands of healthcare workers occurs after contact with a source patient.63
Acinetobacter is easily transmitted from healthcare workers and the general environment, including medical equipment, to patients. The ability to form a biofilm and the presence of dormant cells enables Acinetobacter to survive for several weeks on abiotic surfaces under dry conditions.64 Therefore, thorough disinfection of a potentially contaminated environment is also important, as is the use of a closed tracheal suction system and vascular devices to prevent Acinetobacter contamination.65 Although some studies have demonstrated successful control of infection without isolation of infected or colonized patients,66 implementation of precautions during contact and isolation of patients is generally encouraged.67,68 The use of patients' own equipment might facilitate the control of outbreaks, and the maintenance of a good hand hygiene regimen for healthcare workers is also important.69 Because previous exposure to antibiotics is considered a risk factor for outbreaks and antibiotic resistance, restriction of the use of broad-spectrum antibiotics may also contribute to a reduction in infections.70
Once endemic in a healthcare unit, it is extremely difficult to eradicate A. baumannii. Whether this organism can be reduced by strict infection control measures after becoming endemic is still under debate. A study of ICU patients showed that a multifaceted intervention featuring active surveillance and environmental cleaning resulted in a sustained reduction in the rate of XDR A. baumannii colonization and infection and reduced the cost of antibiotics and hospitalization.71 Further well-designed randomized controlled trials are needed to validate the effects of these strategies in endemic settings.
 XML Download
XML Download