

 PDF
PDF ePub
ePub Citation
Citation Print
Print


WHAT IS YOUR DIAGNOSIS?
A 27-year-old man presented to the emergency department with sudden-onset, massive gross hematuria and oliguria. On admission, his blood pressure was 100/60 mmHg, his body temperature was 36.3℃, his pulse rate was 108 beats/min, and his respiration rate was 20/min. He had no known medical or surgical history or drug history. The relevant laboratory data were as follows: white blood cell count, 19,600/mm3; hemoglobin level, 9.5 g/dl; platelet count, 353,000/mm3; blood urea nitrogen level, 15.3 mg/dl; creatinine level, 1.5 mg/dl; chronic reactive protein level, 1.0 mg/dl. Urine analysis revealed proteinuria (>300 mg/dl), pyuria (100/HPF), and hematuria (100/HPF). The chest PA showed no active lung lesions. We performed Foley catheterization and checked abdominal computed tomography (CT) with intravenous pyelogram (IVP). The contrast-enhanced excretory-phase CT image showed uneven dilated calices (arrows) and a narrowing of the renal pelvis (arrowhead) of the left kidney, and a large hematoma was noted in the urinary bladder (Fig. 1A). On the CT-IVP image, the left pyelonephrogram was not visible in contrast with a normal right pyelonephrogram (Fig. 1B).
THE DIAGNOSIS: GROSS HEMATURIA ASSOCIATED WITH GENITOURINARY TUBERCULOSIS
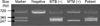
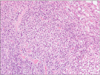
Because a large hematoma was shown in the urinary bladder, we performed an emergency cystoscopy. The cystoscopic findings demonstrated a friable bladder wall and hyperemic mucosal change in the bladder dome. The cystoscopic findings also showed a blood clot near the orifice of the left ureter, which contained an irregular protruding mucosa. A biopsy of this lesion was performed. Acid-fast bacilli staining and culture and urine cytology were checked. Urine acid-fast bacilli staining was negative, but urine polymerase chain reaction (PCR) and culture yielded Mycobacterium tuberculosis (Fig. 2). The chronic granulomatous inflammatory lesion was seen in the biopsy specimen (Fig. 3), and PCR also showed a positive result for M. tuberculosis in paraffin-embedded samples. The large hematoma in the bladder was removed and renal function was recovered. Anti-mycobacterial therapy including isoniazid 300 mg, rifampin 600 mg, and ethambutol 1,200 mg once daily was commenced for 1 year. At 6 months, there were no significant changes in the ureter or bladder wall thickening and dilatation of the calyx on follow-up abdominal CT.
Genitourinary tuberculosis is the second most common clinical manifestation of extrapulmonary tuberculosis.1 Infection is spread either hematogenously to organs such as the prostate gland, seminal vesicles, and kidneys or by direct extension. However, radiographic evidence of pulmonary tuberculosis is present in less than 50% of patients with renal tuberculosis, and active pulmonary disease is present in approximately 5% of such patients.2 The clinical manifestations are variable. The onset of clinically evident genitourinary tuberculosis is insidious with dysuria and gross hematuria. Constitutional symptoms, such as fever, weight loss, fatigue, and poor appetite, are less common.3
Radiologic studies such as IVP are often helpful. The findings of genitourinary tuberculosis depend on the extent of the disease process and may be subtle and difficult to define at an early stage. The earliest renal changes on IVP include erosion of the tips of the calyces, blunting of the calyces, and papillary necrosis.3 Radiological findings in the ureter are variable. Early ureteric infection produces ulcerations. Healing of these ulcers may result in ureteric fibrosis. The urinary bladder may show poor distensibility owing to fibrosis. The definitive diagnosis still rests on microbiological tests such as finding acid-fast bacteria in the urine, urine culture, tissue biopsy, and polymerase chain reaction for M. tuberculosis. The approach to treatment of renal tuberculosis is generally the same as that for pulmonary tuberculosis. The drug regimen varies depending on whether the patient has HIV infection or drug-resistant tuberculosis.

 XML Download
XML Download