

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Statins (3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors) are prescribed worldwide in patients with or at risk for cardiovascular disease (CVD). Reduction of low-density lipoprotein (LDL) cholesterol is one of the primary mechanisms of CVD prevention. Beyond the lipid-lowering effect of statins alone, there is abundant evidence showing that statins provide immediate benefits, the so-called pleiotropic effects of statins. These pleiotropic effects are thought to include improved endothelial function, enhanced stabilization of atheromatous plaque, decreased oxidative stress, decreased vascular inflammation, and a decrease in the probability of developing atherosclerotic events in metabolic syndrome, type 2 diabetes, and hypertension.1-6 These effects of statins may consequently prevent plaque rupture and subsequent myocardial infarction in the proinflammatory and prothrombotic environment.7,8 Recently, randomized controlled clinical trials have raised the concern that lipophilic statins might have unfavorable metabolic effects, such as reducing insulin secretion and exacerbating insulin resistance and the development of new-onset diabetes.3,9,10 Another study also showed that atorvastatin treatment resulted in significant increases in fasting insulin and glycated hemoglobin (HbA1C) levels consistent with insulin resistance in hypercholesterolemic patients.11 These concerns are very important because insulin resistance increases the risk of CVD. Although some studies have been published on the adverse effects of statins, their effects on insulin resistance and new-onset diabetes are not obvious.3,6,11,12
The purpose of this study was to evaluate the effects of rosuvastatin on insulin resistance and adiponectin in patients with newly diagnosed mild to moderate hypertension.
MATERIALS AND METHODS
1. Patients and methods
This study was a randomized, prospective, single-blind study in patients with mild to moderate hypertension [systolic blood pressure (BP)<170 mmHg or diastolic BP<105 mmHg] from September 2009 to April 2010. The study was carried out in Gwangju Veterans Hospital and was approved by the institutional review board of the hospital. Every patient was given full information about the study objectives and methods and signed a written informed consent form. No patient had taken any lipid-lowering agent, hormone therapy, or vitamin supplements during the 8 weeks before randomization. Also, during the pre-randomization period (8 weeks) and the study period, to make the comparison of insulin sensitivity fair in the two groups, all patients took an angiotensin type II receptor blocker (ARB), telmisartan 80 mg, followed by a calcium channel blocker for the treatment of hypertension. Patients with newly diagnosed mild to moderate hypertension were included. We excluded patients with renal disease, hepatic disease, any thyroid disease, uncontrolled diabetes (HbA1C>8%), uncontrolled severe hypertension, stroke, acute coronary syndrome, and unstable angina.
After a 1-week screening period, 57 patients were randomly assigned to either placebo (Group I: mean, 61.5±6.9 years, n=26) or rosuvastatin 20 mg (Group II: mean, 60.4±7.2 years, n=27) once daily during a 2-month treatment period. The allocation was performed by using envelopes. At screening, 57 patients were enrolled in the study. One patient was diagnosed with hepatocellular carcinoma. Three patients withdrew their informed consent. Thus, the final analysis was performed on 53 patients (Fig. 1).
The patients were examined at baseline and at 8-week follow-up visits to assess changes in fasting glucose, insulin, HbA1C levels, QUICKI (quantitative insulin-sensitivity check index), HOMA (homeostasis model assessment), adiponectin, and flow-mediated vasodilation (FMD).
2. Measurement of blood pressure
For BP measurement, stabilization was attempted for more than 10 minutes. BP was measured on the right upper arm with the patient in a sitting position. The measurement was performed at least 2 times at a minimum interval of 10 minutes and the measurements were averaged. Systolic BP of more than 140 mmHg or diastolic pressure of more than 90 mmHg was defined as hypertension.
3. Evaluation of vascular endothelial function
The evaluation of vascular endothelial function was performed by FMD, a noninvasive method. To ensure that the ultrasonographic findings of the brachial artery were detected, the most accessible area, which was 2 to 5 cm inferior to the antecubital fossa, was targeted by use of a high-resolution ultrasonography unit (Sequoia 512; Acuson, Mountain View, CA, USA) to which a 10 MHz linear array transducer was implanted. Ultrasonography was performed according to methods reported previously.13,14
4. Insulin resistance and adiponectin measurement
Blood sampling was done in the morning before treatment and after 8 weeks of drug administration and more than 8 hours of fasting. Plasma insulin was measured with a radioimmunoassay (Biosource Inc., Nivelles, Belgium), as was adiponectin (LINCO Research Inc., St. Louis, MO, USA). Indices for insulin sensitivity (QUICKI and HOMA) were calculated on the basis of the following formulas: QUICKI=1/{log (insulin)+log (glucose)} and HOMA=fasting insulin × fasting glucose/22.5. The units of measurement of insulin and glucose were µU/ml and mg/dl, respectively.
5. Statistical analysis
All data are expressed as the mean±SD. We used Student's paired t test or Wilcoxon signed rank test to compare values between baseline and treatment at 2 months. A comparison of the measurements between the two groups was made by using repeated-measures ANOVA. The mean delta change (%) was calculated as a mean of delta change=(baseline value - follow-up value)/baseline value × 100 (%). All statistical procedures were performed with the Statistical Package for the Social Sciences (SPSS), version 13.0 (SPSS Inc., Chicago, IL, USA). A p<0.05 was considered statistically significant.
RESULTS
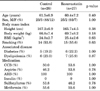
The baseline characteristics of the subjects are shown in Table 1. No significant differences existed between the two treatment groups. There were 48 men and 5 women; the patients' mean age was 60.7±6.8 years. Fourteen of the patients had type 2 diabetes. None of the patients experienced any drug-related complications during the 8 weeks of treatment.
Both groups showed significant improvements in systolic blood pressure (control group, from 153.4±14.7 mmHg to 137.9±14.3 mmHg; rosuvastatin group: from 154.4±14.3 mmHg to 132.8±13.8 mmHg; p<0.01) and FMD (control group, from 7.5±3.1% to 9.9±2.9%; rosuvastatin group, from 7.8±3.5% to 10.5±3.6%; p<0.01) after 8 weeks compared with baseline. However, there were no significant differences between the two groups after 8 weeks of treatment (Table 2). The control group did not show significant changes in the lipid profile, but the rosuvastatin group showed improvement in total cholesterol (from 218.2±36.9 mg/dl to 167.1±43.0 mg/dl; p<0.01), LDL-cholesterol (from 147.5±33.3 mg/dl to 101.8±32.4 mg/dl; p<0.01), and triglycerides (from 174.0±61.9 mg/dl to 136.8±64.6 mg/dl; p<0.01; Table 2). Neither group showed a significant change in the high-sensitivity C-reactive protein level from baseline to 8 weeks.
There were no significant differences in fasting glucose, fasting insulin, QUICKI, HOMA, or adiponectin levels between the two groups before or after randomization (Table 2). The mean delta changes in HbA1c (3.0±10.1% vs. -1.3±12.7%; p=0.33), fasting glucose (-1.3±18.0% vs. 2.5±24.1%; p=0.69), and fasting insulin levels (5.2±70.5% vs. 22.6±133.2%; p=0.27) in the control and rosuvastatin treatment groups were not significantly different (Fig. 2). Furthermore, the mean delta changes of the QUICKI (2.2±11.6% vs. 3.6±11.9%; p=0.64) and HOMA index (11.6±94.9% vs. 32.4±176.7%; p=0.44) also were not significantly different between the control and rosuvastatin groups (Fig. 3). The plasma adiponectin level increased significantly in both groups compared with baseline. However, there was no significant difference in the mean delta change between the control and rosuvastatin groups (23.2±28.4% vs. 23.1±27.6%; p=0.36; Fig. 4).
DISCUSSION
The current study showed that 8 weeks of rosuvastatin (20 mg daily) therapy resulted in no significant improvement or deterioration in fasting glucose levels, adiponectin levels, or insulin resistance. As expected, all components of the lipid profile improved more from baseline following rosuvastatin treatment than control treatment. Our results suggest that rosuvastatin did not cause glucose intolerance or insulin resistance.
Insulin resistance is associated with increased risk for CVD.15,16 The association between insulin resistance and hypertension is controversial. Whereas some studies have reported that insulin resistance is strongly related to hypertension, others have shown only a weak or even no association.17-19 In clinical practice, risk factors for CVD tend to cluster within individuals, and hypertensive patients are at increased risk for metabolic syndrome and adverse changes in insulin resistance and the lipid profile. For risk modification, statins are prescribed in patients with multiple risk factors for CVD.
Recent clinical studies have demonstrated that lipophilic statins, such as atorvastatin, simvastatin, and the hydrophilic statin rosuvastatin might increase the onset of new diabetes.3,9,10 However, these studies were not designed to evaluate the onset of new diabetes or insulin resistance. Therefore, these results are not clear and have not led to recommendations for the general population. Other researchers have previously reported that simvastatin reduces adiponectin levels and insulin sensitivity.20 Previously, Koh et al.11 published that atorvastatin treatment in healthy hyperlipidemic patients aggravates insulin resistance by increasing fasting glucose, insulin, and HbA1c levels at relatively high doses. The characteristics of the patients in both studies were similar. The baseline characteristics, such as lipid level, proportion of diabetic patients, and laboratory findings of baseline insulin resistance were similar, even though the patient group in that study was composed of healthy volunteers and our patient group consisted of newly diagnosed hypertensive, dyslipidemic patients.11 Indeed, whether statins, especially atorvastatin, have a decisive effect on insulin resistance is unclear. Recently, Koh et al.21 published that compared with pravastatin, rosuvastatin therapy significantly increased fasting insulin and HbA1c while decreasing plasma adiponectin levels and the QUICKI index compared with baseline. A reason may exist for this discordance. First, our patients simultaneously took telmisartan 80 mg, which has a PPAR-γ effect that improves insulin resistance. As a result, it follows that it may have had some masking effects. This is a limitation of our study protocol. Second, our study groups consisted of hypertensive, dyslipidemic patients and included some patients with diabetes. Our patients already had metabolic disease. Thus, the unwanted metabolic effect by rosuvastatin may have been relatively weaker than in the patients in Koh et al.'s study.
Huptas et al.6 showed that 6 weeks of atorvastatin treatment results in significant improvement in insulin sensitivity in patients with metabolic syndrome. But, these conflicting results cannot be explained. Furthermore, it is unknown whether different statins have different metabolic effects on the basis of their lipophilic properties. Similar findings were shown for pravastatin, which is nonlipophilic.22,23 Another study compared the effects of atorvastatin (10 mg) and rosuvastatin (10 mg) on changes in glucose and insulin levels, and the HOMA of the insulin resistance index, which were not significantly different between the two groups.24 Also, the result of a meta-analysis of randomized controlled trials may suggest that potential differences exist between statins.25 It is not clear why various statins have beneficial metabolic actions in some studies, but not in others. Thus, further head-to-head comparative studies are needed to elucidate the effects of statins on glucose metabolism.
Our results showed that lipid levels improved, adiponectin levels increased, and the percentage change in fasting glucose and insulin levels and the QUICKI and HOMA indexes were not significantly different between the rosuvastatin and control treatment groups. To determine the trends in each group's differences according to treatment, we assessed the mean value of each parameter and the mean of the delta change. The values shown in Table 2 and the mean change percentages (Fig. 2-4) for each parameter may seem to be different results. But this could be because of the statistical differences. Studies in an animal model of insulin resistance suggested that rosuvastatin treatment increases whole-body and peripheral tissue insulin sensitivity via improved cellular insulin signal transduction.26 A 20 mg dose of rosuvastatin, which is a relatively high dose, was used in our study. Rosuvastatin (20 mg) has equal lipid-lowering potency as atorvastatin (40 mg). Therefore, we assume that each statin has differential effects on insulin sensitivity and the rate of new-onset diabetes according to dosage.
The rosuvastatin (20 mg) group tended to show improved vascular endothelial function and FMD, but showed no significant difference at the time of study termination. Our study and another study showed that treatment with a statin improved FMD in patients with a decreased baseline FMD.27 In that study, discontinuation of statin treatment reversed the improved FMD to baseline.27 The results showed that statins definitely affect vascular endothelial function, but only in patients with increased cardiovascular disease risk factors. In the current study, most patients had low cardiovascular disease risk factors; the anti-hypertensive ARB therapy could have already resulted in maximum improvement of vascular endothelial function. Under such conditions, statins would not have an additional effect on vascular endothelial function owing to the ceiling effect. If the current study had enrolled more patients with diabetes, metabolic syndrome, or other cardiovascular disease, the results would possibly have greater meaning.
In our data, the value of adiponectin increased in both groups but did not differ significantly between the two groups. Some diabetic patients were included in this study, because many hypertensive patients already show metabolic disease in the real world. As a natural consequence, it follows that analysis of our data was partially ambiguous. Furthermore, telmisartan 80 mg, which has a PPAR-γ effect that improves insulin resistance, was taken by all patients for adequate BP control. As a result, it follows that the ARB may have shown good BP control but some masking effects on adiponectin, inflammatory markers, and insulin resistance.
In conclusion, our study showed that 8 weeks of rosuvastatin (20 mg daily) therapy showed no significant improvement or deterioration of fasting glucose levels, insulin resistance, and adiponectin levels in newly diagnosed hypertensive patients treated with the ARB telmisartan.





 XML Download
XML Download