

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Over recent decades, drug-eluting stents (DES) have emerged as the preferred treatment for coronary artery disease, and the use of DES has increased significantly. The use of DES reduces the rates of restenosis by inhibiting neointimal hyperplasia. However, accumulating evidence suggests that DES may increase the rate of late thrombosis, and stent implantation causes endothelial denudation, medial dissection, and exposure of the subintima, which leads to subsequent platelet activation. Current treatment with DES for coronary artery disease is very promising, but has the drawback of late in-stent thrombosis, delayed re-endothelialization, and polymer-mediated inflammation.1
Statins have a beneficial effect on not only coronary endothelial cells but also endothelial progenitor cells (EPCs).2-4 Moreover, statins have pleiotropic effects, which include the inhibition of neointimal hyperplasia, the inhibition of vascular inflammation, and platelet inhibition.5 Therefore, we hypothesized that statin-eluting stents may improve the impaired re-endothelialization and inhibit the neointimal hyperplasia after stenting.
This experiment was a preliminary study conducted in the development of a novel dual-drug layer or dual-drug mixed coating stent with an antiproliferative agent such as paclitaxel and sirolimus and a drug to treat delayed arterial healing. In the present study, we investigated the efficacy of an atorvastatin-eluting stent (AES) compared with a paclitaxel-eluting stent (PES) in rabbit iliac arteries.
MATERIALS AND METHODS
1. Animal preparation
All experimental procedures and protocols used in this investigation were approved by the Ethics Committee of Chonnam National University Medical School and Chonnam National University Hospital (CNU IACUC-H-2010-16) and conformed to the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85-23, revised 1996). To prevent acute thrombosis after stenting, premedication with aspirin 20 mg per day was given for at least 4 days before the procedure.
2. Study groups
The rabbits were randomly divided into 2 groups (Table 1): group 1 (AES, n=10) and group 2 (PES, n=10). A total of 10 rabbits were used in this study (10 rabbits, 20 iliac arteries, 10 iliac arteries in each group). An AES and a PES were implanted in the right iliac artery and left iliac artery in a randomized manner in each rabbit.
3. Preparation of atorvastatin- or paclitaxel-eluting stents
We used our developed bare metal stent (CNUH stent) as previously reported.6 The atorvastatin- and paclitaxel-loaded biodegradable PLGA [poly(lactic-co-glycolic acid)] coatings were fabricated onto the surface of the bare metal stents (CNUH stent, 3.0×18 mm, Co-Cr alloy, L605) by using an ultrasonic atomization spray method.7 The AES with 200 µg atorvastatin and PES with 177 µg paclitaxel were prepared.
4. Rabbit iliac artery stent implantation
Male New Zealand white rabbits (n=10) weighing approximately 3.5 kg were used. Stent implantation was performed under sterile conditions by using portable fluoroscopic imaging (BV Pulsera, Philips). Rabbits were anesthetized intravenously through the right marginal ear vein with a mixture of xylazine (2.2 mg/kg) and ketamine (22 mg/kg). Body temperature was controlled at 37℃ through the use of a heating pad and the animals received supplemental oxygen continuously through an oxygen mask. Continuous hemodynamic and surface electrocardiographic monitoring was maintained throughout the procedure.
Subcutaneous 2% lidocaine was administered at the cut-down site. An incision was made above the right carotid artery and the vessel was dissected free. A 4-Fr introducer sheath (Radifocus Introducer 2, Terumo Co, Tokyo, Japan) was inserted into the vessel, preloaded with a guide wire (Radifocus, Terumo Co, Tokyo, Japan), and advanced from the carotid artery into the distal descending aorta. The guide wire was then advanced to the proximal portion of the iliac artery. The stent delivery system was advanced to the distal portion of the iliac artery by using the guide wire and the stent was deployed to a pressure of 8 atm to achieve a stent-to-artery size ratio range of 1.3:1.8 Intravenous heparin (100 U/kg) was administered immediately after stent deployment.9 Successful deployment was verified by angiography, and the introducer sheath was removed. The right carotid artery was ligated, the incision above the carotid artery was closed in layers, and the rabbit was allowed to emerge from anesthesia. Rabbits received antibiotic prophylaxis (enrofloxacin, 5 mg/kg) for 4 days after stent implantation and aspirin in their drinking water (20 mg/day) for the duration of the protocol.9 Four weeks after stenting, the animals underwent follow-up angiography in the same views as before and were sacrificed by injection with 20 mL of potassium chloride through the left carotid artery.
The stented iliac arteries were pressure-perfusion fixed at 110 mm Hg in 10% neutral buffered formalin overnight. Arteries were step-sectioned, processed routinely for light microscopy, and stained for histological analysis.
5. Histological analysis
Rabbits underwent iliac artery stent implantation as described above and were sacrificed 28 days after deployment. Histopathologic evaluation of each iliac artery was performed by an experienced cardiovascular pathologist. The specimens were embedded and sections of 50 to 100 µm thickness were obtained at about 1 mm apart and stained with hematoxylin-eosin (Fig. 1) and Carstairs' stain (Fig. 2) for histological analysis. Measurements of the histopathologic sections were performed by using a calibrated microscope, digital video imaging system, and microcomputer program (Visus 2000 Visual Image Analysis System, IMT Tech). Borders were manually traced for lumen area, area circumscribed by the internal elastic lamina, and the innermost border of the external elastic lamina (external elastic lamina area). Morphometric analysis of the neointimal area for a given vessel was calculated as the measured internal elastic lamina area minus the lumen area. The measurements were made on five cross-sections from the proximal and distal ends and the three midpoints of each stented segment. Histopathologic stenosis was calculated as 100×[1-(lesion lumen area/lesion internal elastic lamina area)].10
6. Evaluation of arterial injury
Arterial injury at each strut site was determined by the anatomic structures penetrated by each strut. A numeric value was assigned as previously described by Schwartz et al.10 0=no injury, 1=break in the internal elastic membrane, 2=perforation of the media, and 3=perforation of the external elastic membrane to the adventitia. The average injury score for each segment was calculated by dividing the sum of injury scores by the total number of struts at the examined section.
7. Evaluation of inflammation score and fibrin score
With regard to the inflammation score for each individual strut, the grading was as follows: 0=no inflammatory cells surrounding the strut; 1=light, noncircumferential inflammatory cells infiltrate surrounding strut; 2=localized, moderate to dense cellular aggregate surrounding the strut noncircumferentially; and 3=circumferential dense inflammatory cell infiltration of the strut. The inflammation score for each cross-section was calculated by dividing the sum of the individual inflammation scores by the total number of struts at the examined section.11 Ordinal data for fibrin were collected on each stent section by using a scale of 0 to 3 as previously reported.12
8. Statistical analysis
Statistical analysis was performed with the aid of commercially available software (SPSS Version 15; Chicago, IL, USA). The data were presented as mean value±SD. Unpaired Student's t-test was used for the comparison of the two stent groups. A value of p<0.05 was considered statistically significant.
RESULTS
1. In vitro DES with atorvastatin or paclitaxel
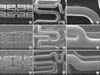
The morphology of the stent surface was smooth and uniform as shown by scanning electron microscope findings. There was no destruction or delamination on the stent coating surfaces (Fig. 3). Drug release graphs showed that about 60% of the atorvastatin and 65% of the paclitaxel were released from the stent over the first 3 days. The drug release was maintained for 4 weeks in both stents (Fig. 4).
2. Analysis after stenting
Two stents were placed in two iliac arteries per rabbit. A total of 20 stents including 10 AESs and 10 PESs were randomly placed in the left and right iliac arteries of 10 rabbits. Mortality for this study was zero. There was no significant difference in stent-to-artery ratio between the two stent groups.
3. Histopathological analysis
There were no significant differences in the injury score (1.2±0.43 in the AES group vs. 1.3±0.45 in the PES group), lumen area (3.9±0.54 mm2 in the AES group vs. 3.7±0.63 mm2 in the PES group), or inflammation score (1.1±0.15 in the AES group vs. 1.1±0.10 in the PES group).
There were significant differences in the internal elastic lamina (4.6±0.46 mm2 in the AES group vs. 4.2±0.55 mm2 in the PES group, p<0.05), in the neointimal area (0.7±0.18 mm2 in the AES group vs. 0.4±0.25 mm2 in the PES group, p<0.01), in the percentage stenosis area (14.8±5.06% in the AES group vs. 10.5±6.80 mm2 in the PES group, p<0.05), and in the fibrin score (0.4±0.51 in the AES group vs. 2.7±0.48 in the PES group, p<0.001) (Fig. 5).
DISCUSSION
The results of this study demonstrated that the AES showed a better arterial healing effect than the PES, which used an anticancer agent such as Taxol and the same polylactic-co-glycolic acid polymer. Although the AES did not show better inhibition of neointimal hyperplasia compared with the PES, the percentage stenosis area value of the AES was effective. The AES is difficult to commercialize by itself, but we developed a novel dual-drug layer or dual-drug mixed coating stent on the basis of the data obtained in this study.
The rabbit iliac artery was selected for stent implantation because the diameter and length of this vessel closely approximate the size of stents frequently used in clinical settings. The absence of axial curvature in these arteries and the ability to obtain coronary stent experimental and control data in the contralateral iliac arteries of a single animal are also important benefits of this model.13 The rabbit iliac artery restenosis model is commonly used in the estimation of DES.
Statins, or 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors, are potent lipid-lowering agents that have been shown to reduce cardiovascular events including myocardial infarction and death.14 Other reports suggest that statins have potent pleotropic effects beside their lipid-lowering effects. Statins have been shown to reduce inflammatory response and oxidative stress, protect vascular endothelial function, and inhibit platelet aggregation.15 Fluvastatin has been shown to accelerate re-endothelialization delayed by local sirolimus treatment with beneficial effects on migration and proliferation of mature endothelial cells.16 Moreover, several studies have shown that statin therapy reduces the incidence of coronary events after stenting.17-19 Atorvastatin, which was used in our study, has been shown to reduce thrombin generation and the expression of glycoprotein IIIa, tissue factor, and P-selectin on platelet-derived microparticles.20
A previous study reported that a cerivastatin-eluting stent shows effective neointimal inhibition with less arterial wall toxicity as well as preserved vasomotor function compared with a PES in rabbit iliac arteries.21 In several other preclinical studies, statin-eluting stents showed beneficial results on restenosis22 and re-endothelialization23 relative to a bare metal stent. The basis for this benefit is a mechanism of early acute direct activation of endothelial nitric oxide synthase, which is neither cholesterol nor HMG-CoA reductase dependent.24 We suspect that statins suppress the delayed arterial healing effect of the Taxol family and -limus derivatives.
Drug-eluting stents coated with an anti-cancer agent such as paclitaxel have been shown to inhibit neointimal proliferation.25 However, the cytotoxicity of paclitaxel may lead to increase in the incidence of late stent thrombosis.26 In a porcine coronary restenosis model, a commercial paclitaxel-eluting stent with a durable polymer inhibited neointima proliferation, but resulted in poor endothelialization and a greater inflammatory reaction than with bare metal stents.27 Thus, DES delivering one of the potent statins with a biodegradable polymer such as PLGA would be a way to address this problem. Furthermore, a statin-eluting stent would not necessitate a change in oral statin dosing because the statin would be administered locally without systemic effects. Therefore, vulnerable lesions not being stented would continue to receive the benefits of statins administered orally.28
1. Study limitations
Our study had some limitations. First, we used normal rabbit iliac arteries without atherosclerotic lesions, which is unlike the human clinical situation with preexisting atherosclerosis. Second, we examined the inflammatory reaction on the basis of H&E staining. Immunohistochemistry techniques are the standard for such studies.29
In conclusion, this study showed that although the AES did not suppress the neointima hyperplasia compared with the PES, which used a cytotoxic anticancer agent, it showed a superior arterial healing effect in a rabbit iliac artery overstretch restenosis model.





 XML Download
XML Download