

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Statins are very well known to reduce cardiovascular events and mortality in patients with coronary artery disease or at high risk of cardiovascular disease. Besides lowering low-density lipoprotein (LDL)-cholesterol, statins have pleiotropic effects such as improved endothelial function, reduced inflammation, and reduced thrombus formation. Many recent studies have demonstrated the efficacy of statins in patients with coronary artery disease. In this article, we review the current evidence for the beneficial effect of statins in patients with coronary artery disease and the questions and problems associated with the adverse effects of statins.
EFFECTS OF STATIN THERAPY IN PATIENTS WITH CORONARY ARTERY DISEASE
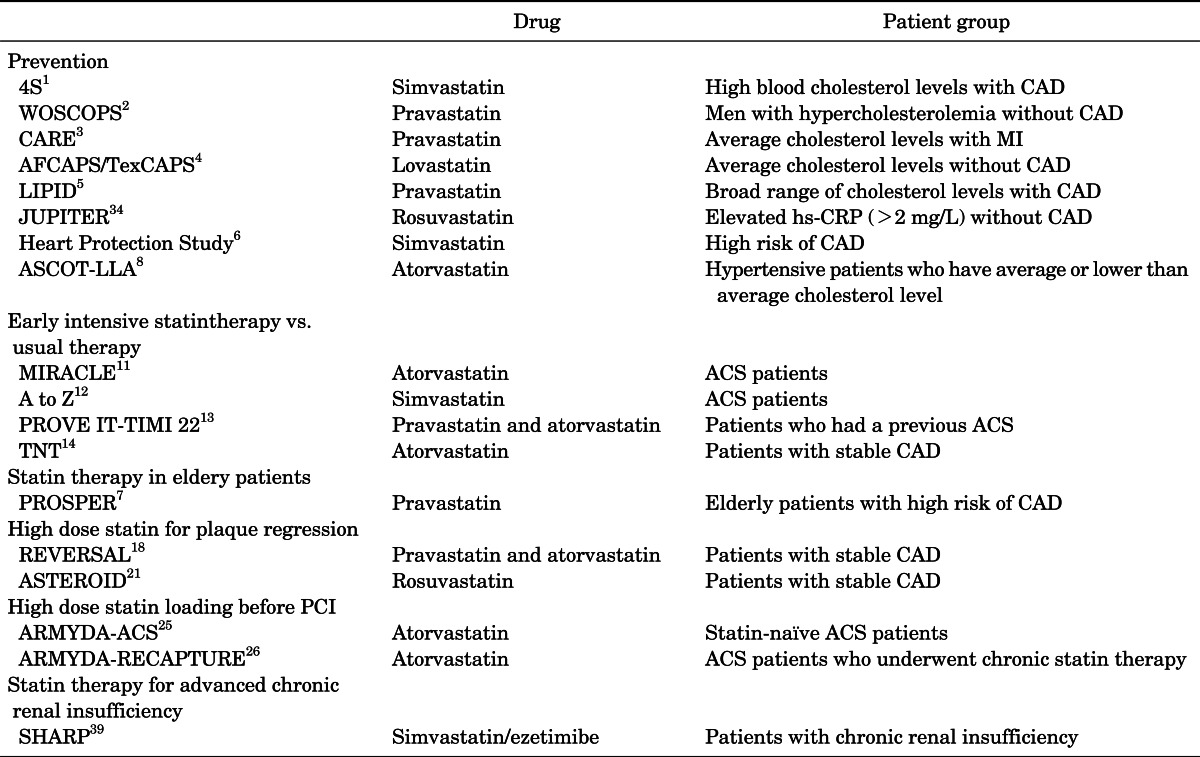
Statins inhibit 3-hydroxy-methylglutaryl coenzyme A (HMG-CoA) reductase, which is responsible for the reduction in the serum low-density lipoprotein (LDL)-cholesterol level. Since the introduction of statin in 1987, many clinical studies have reported that statin therapy reduces major cardiovascular events by reducing the LDL-cholesterol level, which led to a revolution in the management of cardiovascular disease. The Scandinavian Simvastatin Survival Study (4S) was the first large-scale study showing that using statins reduced major cardiovascular events, cardiovascular mortality, and total mortality in patients with coronary artery disease and high blood cholesterol levels.1 Then, the West of Scotland Coronary Prevention Study (WOSCOPS) showed that statins reduce major cardiovascular events and cardiovascular mortality in patients with high blood cholesterol levels but without coronary artery disease.2 In the Cholesterol and Recurrent Events (CARE) trial, the cardioprotective effects of statins were also demonstrated in patients with myocardial infarction and average cholesterol levels.3
The statins also have demonstrated efficacy in patients with a broad range of initial cholesterol levels but without coronary artery disease and in patients with average cholesterol levels and coronary artery disease.4,5 Statins have also been shown to significantly reduce cardiovascular clinical events in a variety of patients, ranging from those with established cardiovascular disease to those who are at risk for cardiovascular disease, in large clinical studies such as the Heart Protection Study of cholesterol-lowering with simvastatin in 20,536 high-risk individuals,6 a study of pravastatin in elderly individuals at risk of vascular disease,7 and the Anglo-Scandinavian Cardiac Outcomes Trial Lipid-Lowering Arm (ASCOT-LLA).8 A meta-analysis of primary and secondary prevention trials of statin therapy demonstrated a 20% reduction of major cardiovascular events and stroke per 1-mmol/L reduction in LDL-cholesterol levels.9 There was also a linear relationship between the reduction in major cardiovascular events and the LDL-cholesterol level in secondary prevention studies using statins.10
Moreover, intensive statin therapy provides more significant clinical benefit than does usual therapy. The Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering study reported that 80 mg atorvastatin within 24 to 96 hours after hospital admission reduced the risk of the composite primary endpoint of death, myocardial infarction, cardiac arrest, and recurrent ischemia by 16% compared with placebo.11 The Z phase of the Aggrastat to Zocor (A to Z) trial showed reducing events after 6 months of treatment in patients with lower LDL levels (66 mg/dl vs. 81 mg/dl).12 The Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 (PROVE IT-TIMI 22) trial showed that intensive therapy achieved results superior to those of standard therapy (median LDL-cholesterol level, 62 mg/dl vs. 95 mg/dl) for reducing clinical events in patients who had a previous acute coronary syndrome.13 This "lower is better" hypothesis is consistent with the results of other trials. The Treating to New Targets (TNT) trial showed fewer major adverse cardiac events in stable patients treated with 80 mg of atorvastatin than in those treated with 10 mg of atorvastatin.14 Thus, the NCEP ATP III and the recent ACC/AHA guidelines recommend that target LDL-cholesterol levels should be below 70 mg/dl for patients with coronary artery disease or for patient with the equivalent of coronary artery disease.15,16
Intensive lipid-lowering therapy with statins not only improves survival rates and clinical outcomes but also reduces the progression of atherosclerosis.17-20 The recent REVERSal of Atherosclerosis with Lipitor (REVERSAL) study showed that progression of the atheroma plaque volume was less with an aggressive dose of statin than with a moderate dose of statin.18 Another study, the ASTEROID (A Study to Evaluate the Effect of Rosuvastatin on Intravascular Ultrasound-derived Coronary Atheroma Burden) trial, demonstrated that intensive statin therapy with 40 mg rosuvastatin daily could induce regression of coronary atherosclerosis. Furthermore, a very strong linear relationship was found between the LDL-cholesterol levels achieved and the course of atherosclerosis.21
Statin therapy before percutaneous coronary intervention (PCI) has been shown to reduce the incidence of periprocedural myocardial necrosis and to improve outcomes.22 Briguori et al.23 reported that the incidence of CK-MB elevation after PCI was approximately 50% lower in patients previously treated with statin than in statin-naïve patients. Furthermore, a meta-analysis showed that statin pretreatment in patients with stable angina resulted in a relative reduction in procedural myocardial necrosis and overall major adverse cardiac events.24 Recently, short-term and high-dose statin pretreatment before PCI showed not only reduced peri-procedural myocardial necrosis and improved outcomes25,26 but also reduced contrast-induced nephropathy after PCI.27
The beneficial effects of statins were also demonstrated in the Korea Acute Myocardial Infarction Registry (KAMIR) study data in patients with low LDL-cholesterol levels28 and in patients with cardiogenic shock.29 Also, Jeong et al.30 reported that statin therapy reduced the incidence of early stent thrombosis in myocardial infarction patients with high levels of high-sensitivity C-reactive protein (>2 mg/L).
Nowadays, statin therapy is widely recommended for the primary and secondary prevention of cardiovascular disease in a wide range of people (Table 1). The benefits of statin therapy are attributed to pleiotropic effects that are independent of a lowering of the LDL-cholesterol level. These effects include improved endothelial function,31 reduced vascular inflammation,32-34 and reduced platelet adhesion and thrombosis.35
Although statin therapy has shown promising effects in the treatment and prevention of cardiovascular disease, some controversies remain concerning the use of statins in patients with chronic renal insufficiency or who are undergoing renal replacement therapy. Some studies showed no significant benefit of statin therapy with regard to a composite cardiovascular endpoint in patients with type 2 diabetes who were undergoing hemodialysis.36,37 In A Study to Evaluate the Use of Rosuvastatin in Subjects on Regular Hemodialysis: An Assessment of Survival and Cardiovascular Events (AURORA), the initiation of treatment with rosuvastatin in patients undergoing hemodialysis lowered the LDL-cholesterol level but had no significant effect on the composite primary endpoint of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke.38 Recently, the SHARP (Study of Heart and Renal Protection) trial showed that reduction of LDL-cholesterol with simvastatin 20 mg plus ezetimibe 10 mg daily safely reduced the incidence of major atherosclerotic events in a wide range of patients with advanced chronic renal insufficiency.39 Also, Lim et al.40 reported that statin therapy reduced major cardiovascular events in 12,853 acute myocardial infarction patients of the Korea Acute Myocardial Infarction Registry regardless of renal function. However, there are few studies concerning the efficacy of statin therapy in coronary artery disease patients with renal insufficiency. Thus, it remains a considerable question whether lowering LDL-cholesterol and levels of inflammatory markers is of value in patients with advanced chronic disease such as chronic renal insufficiency or heart failure. Larger prospective studies are needed to confirm this issue.
The usually prescribed doses of statins are safe, and complications of statin therapy are very rare. The incidence rate of hepatic toxicity (more than 3 times the upper normal limit of liver enzymes) is less than 1%. In the TNT study, hepatic toxicity was found in 0.2% of patients using 10 mg of atorvastatin and in 1.2% of patients treated with 80 mg of atorvastatin.14 Rhabdomyolysis is considered to be one of the most important complications in the population taking statins.41 However, previous studies have shown that there is a higher incidence of statin-induced rhabdomyolysis when statins are used along with drugs that affect the cytochrome P450 3A4 system, i.e., fibrate, nicotinic acid, cyclosporine, macrolide antibiotics, and others.42 Physicians should advise their patients who are taking statins to be aware of the risk factors for rhabdomyolysis or elevated liver enzymes.
Despite the beneficial effects of statins, some reports have suggested that statins increase cancer risk43 and have an unfavorable effect on glucose metabolism. In the PROSPER study, which was a study of older people, new cancer was diagnosed 25% more frequently in the statin-treated group than in the placebo group.7 However, in most studies with a wide age range of patients, the incidence of cancer was not increased with statin therapy.44,45 There have also been some reports that some lipophilic statins have an unfavorable effect on glucose metabolism. Koh et al.46 reported that atorvastatin might cause unfavorable metabolic effects on glucose metabolism. They reported that 80 mg of atorvastatin treatment resulted in significant increases in fasting insulin and glycated hemoglobin levels consistent with insulin resistance and increased ambient glycemia in hypercholesterolemic patients despite beneficial reductions in LDL-cholesterol. Similar laboratory and clinical data exist showing that some lipophilic statins have an unfavorable effect on glucose metabolism when administered in high doses.47-49 A recent meta-analysis of whether individual statins have differing effects on insulin sensitivity showed that statins do not appear to demonstrate a "class effect" on insulin sensitivity.50 Pravastatin was found to significantly improve insulin sensitivity, whereas simvastatin significantly worsened it. Therefore, statins need to be administered cautiously in patients balancing the risk of diabetes mellitus with the benefit of reducing atherosclerosis. Because a higher dose of statin increases the side effects, the maximal recommended dose is limited to the initial dose for high-risk patients.
CONCLUSION
Statins are very effective and safe drugs for preventing and treating coronary artery diseases regardless of cholesterol levels. However, further research is needed to elucidate whether statins are effective in patients with advanced chronic disease such as chronic renal insufficiency or heart failure. In the field of real clinical practice, statins should be prescribed in all patients with coronary artery disease unless the patient presents with several complications such as rhabdomyolysis or elevated liver enzymes.
 XML Download
XML Download