

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute myocardial infarction (AMI) typically results from critical coronary occlusive diseases or a total coronary occlusion after acute plaque rupture.1 Myocardial infarction with angiographically near-normal coronary arteries (MINC) is a multifactorial syndrome for which the exact cause often remains undetermined in individual patients.2-4 Disparate etiologic factors have been incriminated in MINC, i.e., transient occlusion of the infarct-related artery owing to platelet hyperactivity and thrombosis (hypercoagulability),5-7 coronary artery spasm,8 coronary embolism,9,10 and coronary abnormalities such as myocardial bridges, coronary ectasia, or coronary dissection.11
Whereas the overall prevalence rate of MINC ranges from 1% to 12% depending on the definition,12 its prognosis may vary according to the underlying causes and its definition. The majority of previous studies have shown that the prognosis of MINC is better than that of significant coronary stenosis (MICAS).13-17 However, a recent study showed similar prognosis between patients with MINC and those with one- or two-vessel diseased MICAS.18 Moreover, MINC patients have a substantial risk of subsequent coronary events within the first year.19 The present study was aimed to examine the clinical characteristics and outcomes of MINC patients compared with those of MICAS patients.
MATERIALS AND METHODS
1. Data collection
The study protocol was approved by the ethics committee of the Chonnam National University Hospital. Patients (n=1,220) admitted with AMI including both ST-elevation myocardial infarction (STEMI) and non-STEMI to Chonnam National University Hospital from January 2006 to December 2008 were retrospectively analyzed. The following criteria had to be met for inclusion in the study: 1) satisfied the criteria for AMI as described in the definition section, 2) no prior history of significant coronary artery stenosis as determined by coronary angiography, and 3) cardiac catheterization and coronary angiography performed during admission. Patients who underwent primary thrombolysis were excluded from the study. Patients were classified into two groups according to the presence or absence of significant coronary artery stenosis as follows: Group I (≥50% diameter stenosis, n=1,120) and Group II (<50%, n=100). Clinical characteristics and 1-month and 12-month major adverse cardiac events (MACE) were reviewed. Patient records were assiduously searched for information on possible etiologic factors, including coronary spasm, myocardial bridge, and spontaneous thrombolysis. Group II was then subdivided into two according to the presence or absence of possible underlying etiology as evidenced by angiography: Group II-a (cryptogenic) and Group II-b (associated with possible causative factors such as vasospasm, myocardial bridge, or spontaneous thrombolysis).
The patient characteristics reviewed included their medical history (diabetes mellitus, hypertension, smoking, dyslipidemia, prior AMI, prior angina, prior coronary artery bypass graft, prior percutaneous coronary intervention, and family history), presentation characteristics [systolic blood pressure (SBP) and heart rate], diagnostic electrocardiography (ECG) (ST-segment elevation or depression, Q-wave, T-wave change, and new onset left bundle branch block), laboratory findings [glucose, creatinine clearance, cardiac enzymes, serum cholesterol, high-sensitivity C-reactive protein (hs-CRP), and N-terminal pro-brain natriuretic peptide (NT-proBNP)], and echocardiographic findings [left ventricle ejection fraction (LVEF) <45%], and medications at hospital discharge. Blood samples were drawn during admission with overnight fasting for fasting blood sugar and blood lipid measurements. Clinical, angiographic, and in-hospital outcome data were retrospectively collected by a nurse or research coordinator. Follow-up and outcome data were retrieved from the hospital database and by telephoning the patients or their next of kin with respect to adverse cardiac events, such as death, angina, reinfarction, and heart failure symptoms.
2. Definitions
The diagnosis of myocardial infarction was primarily based on the detection of a rise or fall in cardiac biomarkers (preferably troponin) with at least one value above the 99th percentile of the upper reference limit together with evidence of myocardial ischemia with at least one of the following: symptoms of ischemia, ECG changes indicative of new ischemia (new ST-T changes or new left bundle branch block, development of pathologic Q wave).20 Coronary stenosis was considered significant if it exceeded 50% in one of the three main epicardial vessels or the left coronary artery. Patients without significant stenosis (Group II) were subgrouped into two; those not having possible etiology of AMI (cryptogenic, Group II-a) and those having possible etiology (Group II-b). The etiologies identified by angiography were coronary spasm, spontaneous thrombolysis, and myocardial bridge. Coronary spasm was defined if the result of a ergonovine test was positive or if generalized spastic vessel was relieved by intracoronary nitroglycerin injection; spontaneous thrombolysis was defined if a thrombotic process had already been resolved when catheterization was being done and thus only remnant thrombi were detected on coronary angiography; and myocardial bridge was defined as coronary stenosis more than 50% in the systolic period. Hypertension was diagnosed if the patient had a history of hypertension with ongoing treatment or the admission blood pressure was equal to or greater than 140/90 mmHg; diabetes was diagnosed if fasting serum glucose was greater than 126 mg/dl or diabetes medication was actively utilized. MACE included death and reinfarction.
3. Coronary angiography
Conventional coronary angiography was performed in a standard manner. Standard multiple projections were recorded for the left and right coronary arteries. Following the insertion of the arterial sheath, heparin was administered at the beginning of the procedure. All patients were treated with 300 mg aspirin and were loaded with 300 or 600 mg clopidogrel before coronary angiography, unless contraindicated. Percutaneous coronary intervention was performed by a standard technique through the femoral approach in most cases. Use of stents and adjunctive devices was determined on the basis of individual physician assessments.
4. Statistical analysis
Statistical analysis was performed by using SPSS software, version 17.0. Continuous variables were reported as the mean value±standard deviation (SD) and were compared by using the Mann-Whitney U test or the Student's t test. Categorical variables were compared by using the chi-square test or Fisher's exact test. A multivariate logistic regression analysis was performed to evaluate predictors for 1-year MACE in combined Group I and Group II patients. Subgroup analysis in Group II was performed to evaluate differences in risk factors and incidence of MACE according to the underlying etiology (Group II-a vs. II-b). Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Kaplan-Meier analysis was used to create freedom-from-event survival curves for MACE, and the log-rank test was used for their comparison. A p value < 0.05 was considered statistically significant.
RESULTS
After screening the angiographic data for the 1220 patients presenting with AMI, a total of 100 consecutive patients (59 men and 41 women) fulfilled the angiographic criteria and were included in the final analysis of Group II. Group I comprised 1120 consecutive patients with AMI resulting from CAD who were identified during the same time period. Of 1120 patients in Group II, 662 (59.1%) received percutaneous coronary intervention, 444 (39.6%) received medical treatment, and 19 (1.6%) underwent coronary artery bypass grafting as the main treatment strategy within 1 year.
1. Clinical characteristics and laboratory findings
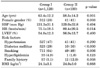
The clinical characteristics are described in Table 1. Group II was younger than Group I (58.5±14.2 vs. 63.4±12.2 years, p=0.001) and included more females (41.0% vs. 28.9%, p=0.008). Group II patients had a lower prevalence of cardiovascular disease risk factors (diabetes mellitus, p<0.001; history of smoking, p=0.005), except for a higher prevalence of a family history of cardiovascular disease. Although a trend toward a lower prevalence of hyperlipidemia was apparent in Group II patients, the difference was not statistically significant. The two groups did not differ significantly with respect to SBP, LVEF, prevalence of hypertension, or body mass index.
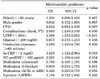
The laboratory findings are described in Table 2. Group II had a higher creatinine clearance rate and lower mean creatine kinase, cardiac enzymes [muscle brain isoenzyme of creatine kinase (CK-MB) and troponin I], low density lipoprotein (LDL)-cholesterol, and apo-B/A1 ratio than did Group I. Blood glucose, total and high-density lipoprotein (HDL)-cholesterol, hs-CRP, NT-proBNP, and Lp (a) levels did not differ significantly between the groups.
2. Etiologic factors related to AMI in Group II
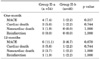
Of the 100 patients (Group II screened), 46 patients (Group II-b) had secondary etiologic factors. A coronary spasm was documented in 29 (29%), myocardial bridge in 11 (11%), and spontaneous thrombolysis in 6 (6%), whereas etiologic factors were not found in the remaining 54 patients (Group II-a). On the other hand, of the 54 patients in Group II-a, stress-induced cardiomyopathy was noted in 15 and myocarditis in 8. LVEF (53.3±13.8 vs. 59.2±13.0%, p=0.014) and creatinine clearance (71.3±33.0 vs. 89.4±32.6 ml/min, p=0.009) were lower, and the levels of NT-proBNP (4,804±7,658 vs. 1,417±3,314 pg/ml, p=0.008) and hs-CRP (3.5±6.8 vs. 0.9±1.3 mg/dl, p=0.023) were higher, in Group II-a than in Group II-b (Tables 3, 4).
3. Etiologic factors tended to elevate cardiac biomarkers without ischemic injury in Group II
Of 100 patients, 7 (7%) had anemia (Hgb < 8 mg/dl), 2 (2%) had severe aortic stenosis, and 3 (3%) had chronic kidney disease (creatinine clearance <30 ml/min). A thyroid function test was done in 25 patients and showed subclinical hypothyroidism in 6 and euthyroidism, although hyperthyroidism was diagnosed before the onset of AMI, in 1.
4. Medications at hospital discharge
Medications at discharge are presented in Table 5. A greater proportion of Group I patients than group II patients were prescribed antiplatelet medications such as aspirin or clopidogrel, beta-blockers, ACE inhibitors, and statin at discharge; a greater proportion of group II patients were prescribed calcium channel blockers. Among discharge medications, aspirin, calcium channel blockers, and ACE inhibitors were associated with 1-year MACE (Table 6).
5. Major adverse cardiac events and all-cause mortality
LVEF (<40%), creatinine clearance (<60 ml/min), hs-CRP (>2 mg/dl), NT-proBNP (>500 pg/ml), and medications (ACEi or ARB) were associated with 1-year MACE in the combined Group I and Group II (Table 7). Clinical outcomes at 1 month and 12 months after the onset of AMI in Group I and Group II are presented in Table 8 and Fig. 1. The 1-year follow up rate was 99.7%. The cumulative MACE rate was 5.0% at 1 month and 9% at 12 months in Group II. The MACE rate did not differ significantly between Groups I and II. Outcomes including mortality and 12-month MACE were also similar between Group II-a and Group II-b (Table 9). Kaplan-Meier death and myocardial infarction-free survival curves up to 1 year revealed a similar survival rate in the two groups (96.0 vs. 97.4%, p > 0.05) (Fig. 1).
DISCUSSION
The present study demonstrated that the prevalence of MINC, defined as a cutoff stenosis limit of 50%, was approximately 8.2% in patients who underwent coronary angiography for indication of AMI. This finding is consistent with prevalences ranging from 1% to 12% of AMI patients, depending on the definition of normal coronary arteries used, i.e., "without any endoluminal irregularity" or "no significant stenosis (<50% stenosis)," in previous investigations.12,17 In addition, our study showed that the outcomes of the patients in Group II were similar to those of Group I patients during the 1-year follow-up, although the patients in the former group were younger, were less likely to have cardiovascular disease risk factors, and had lower cardiac enzymes. Groups II-a and II-b also showed a similar 1-year outcome, although the former had a higher level of NT-proBNP and hs-CRP and a lower LVEF than did the latter.
Most previous studies have demonstrated that MINC patients have lower cardiovascular disease risk profiles and cardiac enzymes than do MICAS patients,12,21-24 whereas others did not find a difference.25 We also found that Group II patients were less likely to have cardiovascular disease risk profiles (i.e., diabetes mellitus, smoking, and LDL-cholesterol levels), except for family history, were more likely to be women, and had lower troponin I and CK-MB levels than did the Group I patients. However, AMI patients with near-normal coronary angiograms in our study tended to be older (mean age 58.5±14.2 years) than were those with near-normal coronary arteries in previous studies,12,21,24 in which age ranged from 42 to 47 years.
Several potential etiologies or mechanisms underlying the occurrence of AMI in patients with near-normal coronary angiograms have been proposed, including concealed atherosclerosis, coronary spasm,8 thrombosis and hypercoagulability,5-7 embolisation,9,10 and inflammation,4 although the eventual etiology remains uncertain in the majority of patients. To determine whether the clinical characteristics and prognosis differed according to the underlying mechanisms, in the present study, we further classified the MINC cohort into 2 subgroups according to their causative pathology: Group II-a (cryptogenic) and Group II-b (with possible etiologies). Our data showed that the possible causative factors in Group II patients were coronary spasm (29%), myocardial bridge (11%), and spontaneous thrombolysis (6%), whereas the causative factors were uncertain in 54% of cases (Group II-a).
We also found that the clinical outcomes of Groups II-a were similar to those of Group II-b; however, serum hs-CRP levels were significantly higher in the former group than in the latter. There is currently abundant evidence linking inflammation with cardiovascular diseases.26,27 hs-CRP is a maker of inflammation that predicts cardiovascular events among healthy individuals.28 In addition, a previous study demonstrated that MINC patients, as compared with MICAS patients, had more frequent febrile infections, mainly of the upper airways, within 2 weeks before AMI, and had a higher seroprevalence of antibodies for Helicobacter pylori, Chlamydia pneumonia, and cytomegalovirus, compatible with an inflammatory component of AMI.29 Moreover, 8 (14.8%) of 54 patients in Group II-a had myocarditis in the present study. Therefore, our finding of increased hs-CRP levels in Group II-a support the previous notion that inflammation may play a role in the pathogenesis of MINC or at least in part contributes to its pathogenesis, although the prevalence of infections was not evaluated in the present study.
NT-proBNP levels were also higher in the Group II-a subgroup. NT-pro-BNP, a cleavage remnant of BNP, is synthesized and secreted by the ventricular myocardium in response to increases in volume or pressure and is known as a predictor of heart failure.30 It has a longer half life than BNP and is renally cleared, thus making it susceptible to significant changes based on alterations in renal function. The increased NT-proBNP level in Group II-a may have been attributed to a reduced left ventricular function, as evidenced by the reduced LVEF, or to decreased renal clearance, as evidenced by the reduced creatinine clearance rate. Indeed, in the present study, 15 (27.8%) of 54 patients in Group II-a had stress-induced cardiomyopathy, which is reported to be associated with marked and persistent elevation of NT-proBNP/BNP levels.31
Although there is general agreement that cardiovascular risk and cardiac enzymes are lower in AMI patients with near-normal angiographic findings, the prognosis of these patients is the subject of some debate.19 Kang et al.18 studied 3,056 patients, of whom 126 (4.4%) had near-normal coronary arteries, and observed a MACE rate including death and reinfarction of 7.8% during 1 year of follow-up in MINC patients vs. 12.2% in comparators with one- or two-vessel disease (p=0.359). Similarly, Group II patients in our study experienced a MACE rate of approximately 9.0% compared with 11.3% in Group I patients (p=0.503) in the first year. Cardiac deaths in 4 patients (4.0%) and noncardiac deaths in 3 patients (3.0%) were the most frequent events in Group II during this follow-up period. These findings indicate that AMI patients with near-normal coronary angiograms experience a significant adverse cardiac event rate and show an overall outcome that is similar to that of MICAS patients within 1 year. However, it has been reported that different degrees of coronary involvement among patients with MINC (a culprit lesion causing <50% angiographic luminal narrowing) show different prognoses, with very few ischemic events in those having strictly normal vessels at long-term follow-up.23,24 Indeed, the prevalence of MINC has fallen to about 1% with advanced diagnostic technologies such as intravascular sonography, multislice computed tomography, and magnetic resonance imaging, and consequently these patients are associated with excellent prognosis.15,32 Therefore, it is likely that the prognosis of MINC patients may differ depending on the definition of MINC with different diagnostic procedures, and those with an absolutely normal coronary artery have a better long-term prognosis than do patients with obstructive coronary artery disease. Nevertheless, the combined morbidity and mortality are not negligible, and thus close follow-up and strict secondary prevention measures, including smoking cessation and prevention of dyslipidemia and diabetes, may be needed in this subset of patients.
The present study had several limitations. First, the data in the present study were retrospectively analyzed in a single center. Angiographic data were harvested from reports available in the cardiac catheterization laboratory database and were largely based on operator description are subject to interobserver descriptive variability. Follow-up data were gleaned from electronic records and in part were obtained by telephone; the accompanying limitations in terms of reliability and accuracy are acknowledged. However, this uncommon condition does not lend itself to randomization and thus charts and angiograms were reviewed. Second, patients in Group I (≥ 50% stenosis) were not further stratified in the present study on the basis of the severity of CAD or the number of vessels involved. Long-term clinical outcomes may differ with different stratification in MICAS and even in MINC.15,26 Third, the time intervals between the onset of chest symptoms and percutaneous coronary intervention were not the same, and the use of thrombolytic therapy before the angiography was not evaluated. The longer the time interval, the more frequently a thrombotic occlusion would have been resolved before catheterization was done, thus resulting in a shift from the MICAS to the MINC group. Fourth, the provocative ergonovine test was not performed in all patients, and the lack of structured workup for hypercoagulable states also limited the ability to systematically analyze the data for etiological factors in Group II. Finally, the small number of patients in Group II and the relatively short duration of follow-up (12 months) might have precluded our ability to detect differences between the groups. Further studies involving a larger number of patients and longterm outcome are needed.
In conclusion, the present study demonstrated that AMI patients with near-normal coronary arteries by angiography have clinical outcomes and prognosis similar to those of AMI patients with occlusive CAD. In addition, 1-year outcomes appear to be similar between MINC patients without and with possible etiologic factors such as coronary spasm, myocardial bridges, and transient thrombosis.







 XML Download
XML Download