

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Infective endocarditis (IE) was described for the first time by Lazare Riviere in 1646, and Osler applied the term malignant endocarditis because the disease was severely fatal.1 IE is an infection of the endothelial surface of the heart and heart valves2 with serious, even fatal, complications and that often requires long-term and expensive treatment.3 IE can be caused by bacteria and fungi, and less commonly, by rickettsiae, chlamydiae, mycoplasmas, and possibly viruses.4 IE has acute and subacute forms, the latter of which may lead to infection of the heart involving damaged endothelium and may occur following dental procedures.5 Dental procedures with tissue injury and bleeding may lead to IE; thus, antibiotic prescription is necessary for high-risk patients, but unnecessary antibiotic prescription may lead to drug resistance, adverse drug reactions, and additional costs to patients.6 Previous reports showed oral bacteria to be the cause of IE in 14% to 20% of cases.7-9 Studies about the knowledge of dentists concerning IE prevention show a low level of knowledge of the current guidelines among Nigerian dentists, especially about correct dose and time of administration.10 Knowledge of dentists and cardiologists and compliance with the available guidelines was also poor.11 Another study reported a relatively high level of knowledge, familiarity with, and acceptance of 2007 guidelines among dentists.12 Lauber showed that clinicians are not always aware of current clinical guidelines, and dentists and physicians exhibit different patterns regarding antibiotic prescription. Dentists were more familiar than physicians with current American Heart Association (AHA) protocols.13
Study about dentists' and dental students' knowledge of the newest guidelines for antibiotic prophylaxis for high-risk patients in dentistry and the correct application of these guidelines in different regions is very important. Limited studies have been performed of these problems in Hamadan. Therefore, one main aim of this study was to evaluate the knowledge of general dentists and final-year dental students concerning the prevention of IE in Hamadan, Iran. Another aim was to compare the knowledge of students and dentists about IE. Thus, each group was evaluated separately, and we also assessed the time separation effect on the mean awareness of students and dentists for their educational needs.
MATERIALS AND METHODS
In this descriptive and cross-sectional study, the awareness of general dentists and dentistry students about prophylaxis against IE was evaluated during 2010. A total of 154 persons participated in this study: 58 were final-year dental students and 96 were Hamadan general dental practitioners. All of the participants were chosen by census sampling methods. All participants were aware of the study goal and those who were not satisfied were excluded. Nameless questionnaires (reliable and valid) were designed and were given to the dentists and students to fill out. A questionnaire was devised that consisted of demographic information such as gender, age, work experience, university from which the dentists had graduated, and questions related to knowledge in three sections.
The first section contained questions pertaining to various cardiac situations and diseases and whether endocarditis prophylaxis was necessary with three choices. The second section contained questions focusing on dental procedures that did or did not require endocarditis prophylaxis with three choices. The questions in the third section included questions regarding the latest endocarditis prophylaxis regimens recommended by the AHA in 2007 with four choices.14,15 In this questionnaire, we used questions from other studies16,17 in addition to some other questions about references for information and the percent of IE that is related to dental procedures (consisting of 31 closed questions in total). The questionnaire is shown in Table 1.
Questionnaire validity, which was approved by 10 dental specialists in different fields of dentistry, and reliability were defined as desirable with statistical analysis. The level of knowledge of the dentists was determined on the basis of the number of correct answers per section. Each correct question was given a score of 1 and each incorrect question and those without an answer were given a score of zero. The total score for awareness was calculated for each participant. A total score under 25% was considered as not at all desirable, a total score of 25% to 49.9% as undesirable, a total score of 50% to 74.9% as relatively desirable, and a total score of 75% and over as desirable. The means of the dentists' and students' knowledge about IE prophylaxis were calculated and the data were compared between the two groups with independent t-tests, chi-square tests, and Mann-Whitney tests by use of the SPSS 16 program. p <0.05 was considered as the level of significance.
RESULTS
This study was performed on 58 senior dental students with a mean age of 29.5±7.7 years (range, 23-45 years), and 96 general dentists with a mean age of 39.8±8.4 years (range, 25-72 years). The dentists' mean work history was 12±7.6 years (range, 1-40 years). Of the total 154 people who participated in this study, 49 (31.8%) were women and 105 (62.2%) were men. The overall knowledge of endocarditis prophylaxis among students and dentists was about 65% and 56%, respectively.
The results showed that 93% of students and 56% of dentists used books as references for information, and there was a statistically significant relation between reference type (source) and knowledge of the two groups (Pearson's chi-square=24.5, p<0.001).
Senior dental students answered more questions about awareness (64.8%), so they had more knowledge than did dentists (56.2%), and this difference was statistically significant (p<0.001). The knowledge of dental students and dentists according to four qualitative descriptors (not at all desirable, undesirable, relatively desirable, and desirable) is shown in Table 2. The students' knowledge was better because 94.9% of students had desired and relatively desired knowledge; however, this result was 82.3% for dentists, and the chi-square test showed a significant relation between groups and knowledge (p=0.013).
The data analysis also showed that gender did not have any effect on knowledge. Knowledge level was not statistically significantly different between women and men (p=0.53).
The results also showed a statistically significant relation among age, graduation year, practice period, and study references with knowledge level (p<0.05). With increasing age, graduation year, and practice period, the level of knowledge was decreased. The group indicating that their references for information were books had more knowledge than did the other groups (Table 3).
Level of awareness about cardiac diseases and dental procedures that need antibiotic prophylaxis are shown in Tables 4 and 5.
Only 28% of students and 36% of dentists selected the correct answer to the question, "What percent of endocarditis is due to mouth bacteria."
Concerning prophylactic treatment, 74% of students and 73% of dentists selected amoxicillin as a choice, 86% of students and 74% of dentists selected 2 g, and 93% of students and 91% of dentists selected 1 hour prior to treatment. In answer to the fifth question, "If we forget to prescribe antibiotics before the dental treatment, is it possible to prescribe after the dental therapy?," 77% of students and 87% of dentists selected the correct answer. For "how long after should antibiotics be prescribed?," 34% of students and 7% of dentists selected the correct answer. For patients with penicillin allergies, 75% of students and 37% of dentists used erythromycin. In answer to the question, "After treatment should patients still be treated with antibiotics?," 37% of students and 51% of dentists prescribed antibiotics after treatment. Among them, 54% prescribed amoxicillin 2 g after treatment, 28% penicillin V every 6 hours per day for 1 week, 11% erythromycin 2 g, and 6% cephalexin every 6 hours for 1 week.
The least knowledge of the students (28%) was about the question "About what percent of endocarditis is due to mouth bacteria?" The least knowledge of the dentists (7%) was about the question "If we forget to prescribe antibiotics before the dental treatment, then for how long after should antibiotics be prescribed?"
DISCUSSION
IE is a severe, life-threatening disease of the heart with poor prognosis. It is difficult to treat and has a high mortality rate. Bacteremia-inducing dental procedures are considered to be one of the major factors.18,19 Thus, an understanding of the various preventative and prophylactic measures is very important in this disease.20 Early diagnosis with prompt treatment with effective antimicrobial therapy is the best way to lower the mortality and morbidity.21 Streptococcus spp. are the main causative microorganisms.4 This study showed that dental practitioners had a moderate level of knowledge (59.4±13.3), but when the data were analyzed in detail, they had poor knowledge about some of these questions. In one study, the overall mean knowledge score of dentists was 37.4±14.3,22 and in another study, the mean knowledge score was 38.77±12.4.23 In the other study, only 40% of dentists were aware of guidelines for IE prevention.18 Thus, the level of awareness was higher in our study than in the above studies.
The overall knowledge of endocarditis prophylaxis among students and dentists was 64% and 56%, respectively. The same results were observed in another study, in which the knowledge level was average (59%). These different results may be related to the study population, time of study, and awareness of dentists in recent years about the significance of IE prophylaxis and studies about it.
Since 2007, new guidelines recommend limiting antibiotic prophylaxis to patients at the highest risk of IE undergoing the highest risk dental procedures.2 Thus, patients with potentially fatal outcomes should receive prophylaxis before dental procedures.24
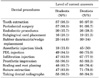
Our results showed that previous endocarditis, prosthetic valves, and rheumatic heart disease, respectively, were the cardiac diseases that most respondents indicated needed antibiotic prophylaxis. The first two answers are compatible with the AHA guideline, but the third answer, rheumatic heart disease, does not match the AHA recommendations.14,15
The study population's knowledge about valve prolapse and rheumatoid fever was lower than their knowledge about the other diseases. Dentists and physicians are not always aware of the most current clinical guidelines regarding antibiotic prophylaxis, even though guidelines are widely available.13
Coutinho et al. studied the knowledge and practices of dentists in preventing IE and concluded that the subjects' knowledge and practices in preventing IE were inadequate.25 The results of a study by Hashemipour et al. showed that previous bacterial endocarditis, rheumatic heart disease, and mitral valve prolapse with valvular regurgitation were diagnosed by dentists to be the most common situations that need antibiotic prophylaxis.22
Most dental procedures that need antibiotic prophylaxis are tooth extraction and periodontal surgery, both of which cause tissue injury and bleeding. Dental procedures that do not need antibiotic prophylaxis are dental radiographs and prosthetic impression, but awareness about endodontic treatment was low.
In another study, removal of calculus was underestimated and bypass overestimated as a risk for bacteriemia, and these errors may lead to overdose or overuse of antibiotics.26 In another study, 43% considered a dental procedure involving any amount of bleeding as being a risk, and only 33% followed the AHA guidelines.25
The most common procedures in which prophylactic antibiotics were distinguished to be necessary were periodontal surgery, scaling, dental extraction, and use of subgingival cords, respectively.23
In this study, 74% of the participants selected amoxicillin as the antibiotic of choice, 76% selected a single 2-g dose, and 91% selected 1 hour before treatment. But in this study, 37% of students and 51% of dentists despite the AHA guidelines administered antibiotics after treatment believing that antibiotics should also be used after treatment.
Only 28% of students and 36% of dentists were aware of the percent of IE caused by oral bacteria.
The least knowledge was about the two questions, "If we forget to prescribe antibiotics before the dental treatment, then for how long after should antibiotics be prescribed?" and "About what percent of endocarditis is due to mouth bacteria?"
In another study also, more than half of the dentists (68.3%) preferred the use of amoxicillin as a prophylactic treatment.22 The decision to use prophylactic antibiotics usually is made by dentists, so they should have enough knowledge about which patients are susceptible to bacterial endocarditis.27
In this study, the association between age and the level of knowledge was also significant, and knowledge decreased as age increased. There was a significant association between the practice period and the level of knowledge; as the work experience of the general practitioner increased, their level of knowledge decreased. Similar results were also observed in another study.20 These associations may be related to aging, time past graduation, and lack of adequate motives for reviewing previously studied sources and taking continuing education courses. This finding is similar to the results of another study that indicated that general dentists and physicians with a practice experience over 20 years had a significantly lower knowledge of endocarditis prophylaxis than did those in practice for less than 20 years. In the study by Eskandari et al, similar results were observed.20
According to these results, more attention should be paid to prophylactic regimens, high-risk patients, and dental procedures that need prophylaxis to prevent IE with a dental source. Also, dentists should be encouraged to educate high-risk patients about the importance of good oral hygiene to prevent unwanted IE in these patients. Revisions should be made in the dental curriculum in the antibiotic prophylaxis field for bacterial endocarditis for students and continuing education programs should be developed to improve the knowledge of dentists regarding antibiotic prophylaxis against IE. Also, other studies should be carried out in the future to study probable differences in correct first-line antibiotic selection among physicians and dentists.13
In our study, the overall awareness level of the study population was moderate. Dentists and students believed that prosthetic valves and previous IE were the most common cardiac diseases that needed prophylaxis. The most common prophylactic regimen was in accordance with AHA guidelines and was a single dose of 2 g amoxicillin 1 hour before treatment. The results indicated that gender had no effect on the level of knowledge, but there was a statistically significant relationship between age and level of knowledge.




 XML Download
XML Download