

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Complications during percutaneous coronary intervention (PCI) include coronary artery complications (perforation, distal embolization, side branch occlusion, and stent thrombosis) and vascular complications (puncture site hematoma, retroperitoneal bleeding, and atheroembolism). Among them, stent entrapment with resulting stent deployment failure is rare but can cause fatal conditions such as stent thrombosis or myocardial infarction.
Although many methods have been used for stent retrieval, there are few reports of the use of a snare via a contralateral femoral approach. Here we report one case of half-degloved stent entrapment that occurred during PCI and that was successfully treated by a snare via a contralateral approach.
CASE REPORT
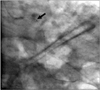
An 80-year-old male was admitted owing to recurrent chest pain for elective PCI of a chronic total occlusion (CTO) in a left circumflex (LCX) lesion. Six months previously, the patient had undergone emergent PCI in the left anterior descending artery (LAD) owing to unstable angina. Follow-up coronary angiography revealed no significant in-stent restenosis in the LAD and CTO in the LCX (Fig. 1). We decided to revascularize the LCX lesion. A 7-Fr JL4 guiding catheter was engaged and predilation with a 2.0×20-mm balloon was done. After ballooning, we attempted to insert the 2.5×30-mm Resolute-Integrity (Medtronic, Minneapolis, MN, USA) stent into the LCX, but the stent failed to cross the CTO lesion in the LCX. We used the deep intubation technique, but the stent could not cross the lesion entirely because the lesion was severely calcified and angulated. While attempting to push the stent, we noticed that the stent was stuck within the lesion. After a struggle, the guiding catheter was taken out but we observed that the stent was half-degloved off the balloon (Fig. 2). Because of the risk of stent loss and embolization, we decided to pull out the catheter and stent strut by use of an Amplatz GooseNeck snare (EV3, Plymouth, MN, USA). We pushed down the guiding catheter and stent strut together to the iliac bifurcation level. The left femoral artery was punctured and we used a 6Fr Balkin sheath to grab the stent with the snare and both the stent strut and the balloon catheter were removed successfully by the snare (Fig. 3). We completed the procedure and decided on medical therapy instead of PCI for the LCX lesion. Two days later, the patient was discharged and there have been no adverse events during 3 months of clinical follow-up.
DISCUSSION
Entrapment of coronary angioplasty devices, especially the stent strut, is rare but is a serious complication of PCI for which cardiac surgery is sometimes required. Calcified, long lesions and angulated lesions may predispose to entrapment of the stent strut. The incidence of stent dislodgement or migration ranges from 1.4% to 8%.1-4 To prevent stent dislodgement or migration, predilatation with a balloon catheter or use of stents with a smaller profile and good tractability are recommended in case of severe angulated or calcified lesions, as in this patient.5
A variety of stent retrieval methods have been described in the literature, such as using a snare device, a multipurpose basket, a variety of forceps, an Angioguard (a distal protection device), a simple balloon and just crushing of the stent into the vessel wall by a balloon.6-10
However, using a balloon or a snare to rescue an entrapped stent in a half-degloved state may contribute to stent loss; to prevent stent loss, it would be safer to approach both sides by inserting the snare via another vascular route.
In this case, we pushed down the stent strut and guiding catheter together to the iliac bifurcation level. After that, the contralateral femoral artery was punctured and both stent strut and balloon catheter were removed successfully by a snare with the aid of a 6Fr Balkin sheath. We think that this technique is safer than other methods in this situation to prevent stent loss and embolization.
However, to avoid serious complications, interventional cardiologists should keep in mind the various complications during PCI and should understand the lesion anatomy and characteristics in their daily practice.


 XML Download
XML Download