

 PDF
PDF ePub
ePub Citation
Citation Print
Print


WHAT IS THE CAUSE OF HER HYPERCALCEMIA AND ERYTHROCYTOSIS?
A 59-year-old female with diabetes mellitus presented with hypercalcemia. Her blood counts were as follows: hemoglobin, 18.2 g/dl; hematocrit, 55.1%; platelets, 361×109/L; and leukocytes, 6.82×109/L. Serum chemistry values were as follows: creatinine, 0.9 mg/dl (normal range, 0.5-1.3); albumin, 5.4 g/dl (4.0-5.2); LDH, 359 IU/L (180-460); ALP, 62 IU/L (104-338); calcium, 12.6 mg/dl (8.6-10.4); and phosphate, 1.9 mg/dl (2.5-4.4). Her serum level of intact parathyroid hormone (iPTH) was increased to 221 pg/ml (normal range, 10-65) and her intact parathyroid hormone-related protein (PTHrP) was below 1.1 pmol/L (normal range, <1.1). The concentration of 1,25-dihydroxyvitamin D3 was 63.54 pg/ml (normal range, 18.7-47.7), calcitonin was below 1.0 pg/ml (normal range, 1.0-4.8), and erythropoietin was 4.3 mIU/ml (normal range, 3.22-31.90). The 24-h urinary concentration of calcium was 820 mg/day and urine output was 3,150 ml. She did not have splenomegaly as shown by abdominal ultrasonography. She underwent neck ultrasonography and Tc-99m sesta-MIBI scanning (Fig. 1).
THE DIAGNOSIS: POLYCYTHEMIA VERA ASSOCIATED WITH PARATHYROID ADENOMA
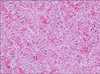
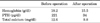
The laboratory data and imaging tests showed hypercalcemia associated with hyperparathyroidism. The patient underwent an operation, and intraoperative exploration of the neck and mediastinum revealed a nodular lesion on the left lobe at the location noted by the parathyroid ultrasonography and scintigraphy. The histopathologic examination of this nodule showed a parathyroid adenoma (Fig. 2). Postoperatively, the patient's PTH dropped to 34 pg/ml and her calcium level was 9.8 mg/dl at 1 month after the operation. Moreover, her hemoglobin and hematocrit dropped dramatically to 15.5 g/dl and 46.7%, respectively (Table 1).
Hypercalcemia in myeloproliferative disorders such as polycythemia vera is usually thought to be related to malignancy, especially renal cell carcinoma.1 Other secondary causes of increased red cell mass are various and include chronic lung disease, smoking, renal artery stenosis, hepatocellular carcinoma, and hydronephrosis.2 However, an association between hyperparathyroidism and polycythemia vera has rarely been reported. In a previous cohort-based study,3 the co-incidence of primary hyperparathyroidism and polycythemia vera was significantly increased, and it was unlikely that this was explained completely by bias or chance. Rather, biologically plausible explanations were identified. The parathyroid tumor may have produced or induced production of a growth factor that can stimulate pancytosis. Moreover, a previous report suggested that the calcium-PTH axis is important for the activation of erythropoiesis,4 but the cause-effect relationship between PTH and myeloproliferative disorders is not yet completely understood. This case demonstrates an association of polycythemia vera and parathyroid adenoma. In conclusion, the differential diagnosis of polycythemia and hypercalcemia should also include the possibility of a parathyroid tumor in addition to other neoplasms.

 XML Download
XML Download