

 PDF
PDF ePub
ePub Citation
Citation Print
Print


WHAT IS THE CAUSE OF RIGHT CEREBELLAR INFARCTION?
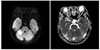
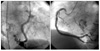
A 76-year-old female presented to the emergency department with the main complaint of 7 days of dyspnea and 1 day of dysarthria and dizziness. She had a history of hypertension. Auscultation findings showed an irregular heart beat with a diastolic rumbling murmur in the apical region and crackles in both lower lung fields. The electrocardiogram showed an irregular pattern corresponding to atrial fibrillation. Brain MRI showed findings compatible with right cerebellar infarction (Fig. 1). Transthoracic echocardiography showed a moderate degree of aortic regurgitation with left ventricular (LV) ejection fraction of 70.8% and a 1.63×1.31-cm complex, echogenic, round, mass-like lesion attached to the left atrial side of the interatrial septum. Transesophageal echocardiography revealed the same mass finding with prominent spontaneous echo contrast in the left atrium and decreased emptying velocity of the left atrial appendage (Fig. 2). The diagnostic coronary angiogram revealed a round, movable mass lesion in the left atrium with feeding arteries originating from the conus branch and atrioventricular nodal artery of the right coronary artery and no significant stenosis in either coronary artery (Fig. 3). The patient was transferred to cardiac surgery and underwent removal of the mass and a Maze operation.
THE DIAGNOSIS: LEFT ATRIAL MYXOMA
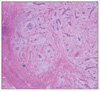
The resected mass had an oval shape and was 2.0×2.0×1.5 cm in size. Macroscopic findings were compatible with myxoma, and the microscopic findings revealed an acid mucopolysaccharide-rich stroma composed of a myxoid matrix and polygonal cells with scant eosinophilic cytoplasm scattered throughout the matrix (Fig. 4). After surgery, the atrial fibrillation was abolished and an electrocardiogram showed a normal sinus rhythm. Follow-up transthoracic echocardiography was performed after surgery and no remnant mass was observed in the left atrium (Fig. 5). At present, the patient is admitted to outpatient department regularly and has taken aspirin and angiotensin receptor blocker steadily without specific problems.
The presence of possible tumor vessels originating from coronary arteries may be helpful in the decision on an operative strategy for cardiac myxoma. About 52% of cardiac myxoma is visualized by coronary angiograms according to previous reports, but catheterization of the chamber from which the tumor arises carries the risk of tumor embolization.


 XML Download
XML Download